Downloaded 134 times




The document discusses the Linate air disaster as an example of organizational errors, highlighting failures at individual, organizational, and inter-organizational levels. Key issues included inadequate communication, lack of proper safety equipment, and non-compliance with international standards, all of which contributed to the tragedy. It emphasizes the need for a just culture that focuses on learning from errors rather than assigning blame.
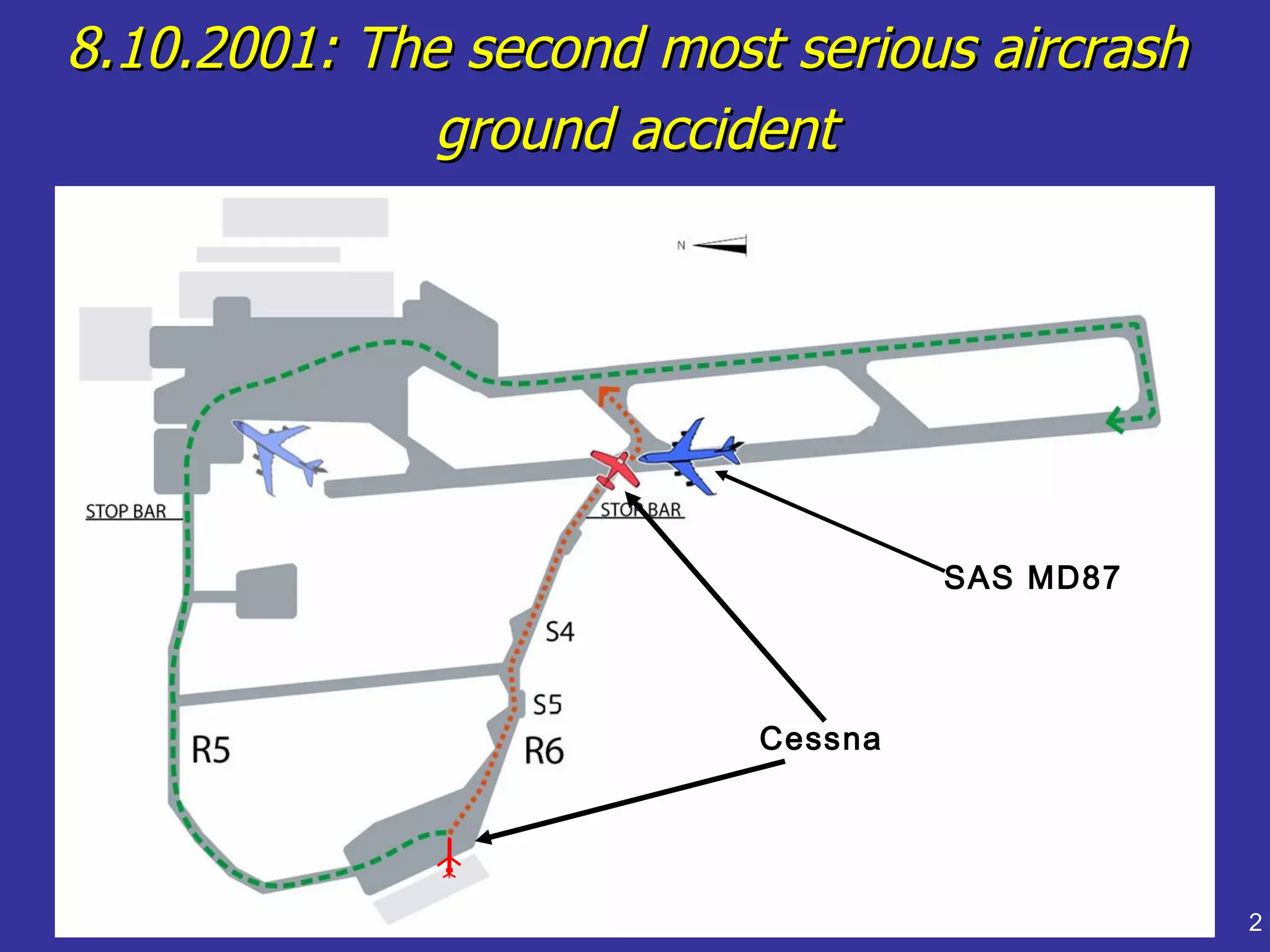
Overview of the Linate air disaster and presentation details. Highlights event date and basic information.
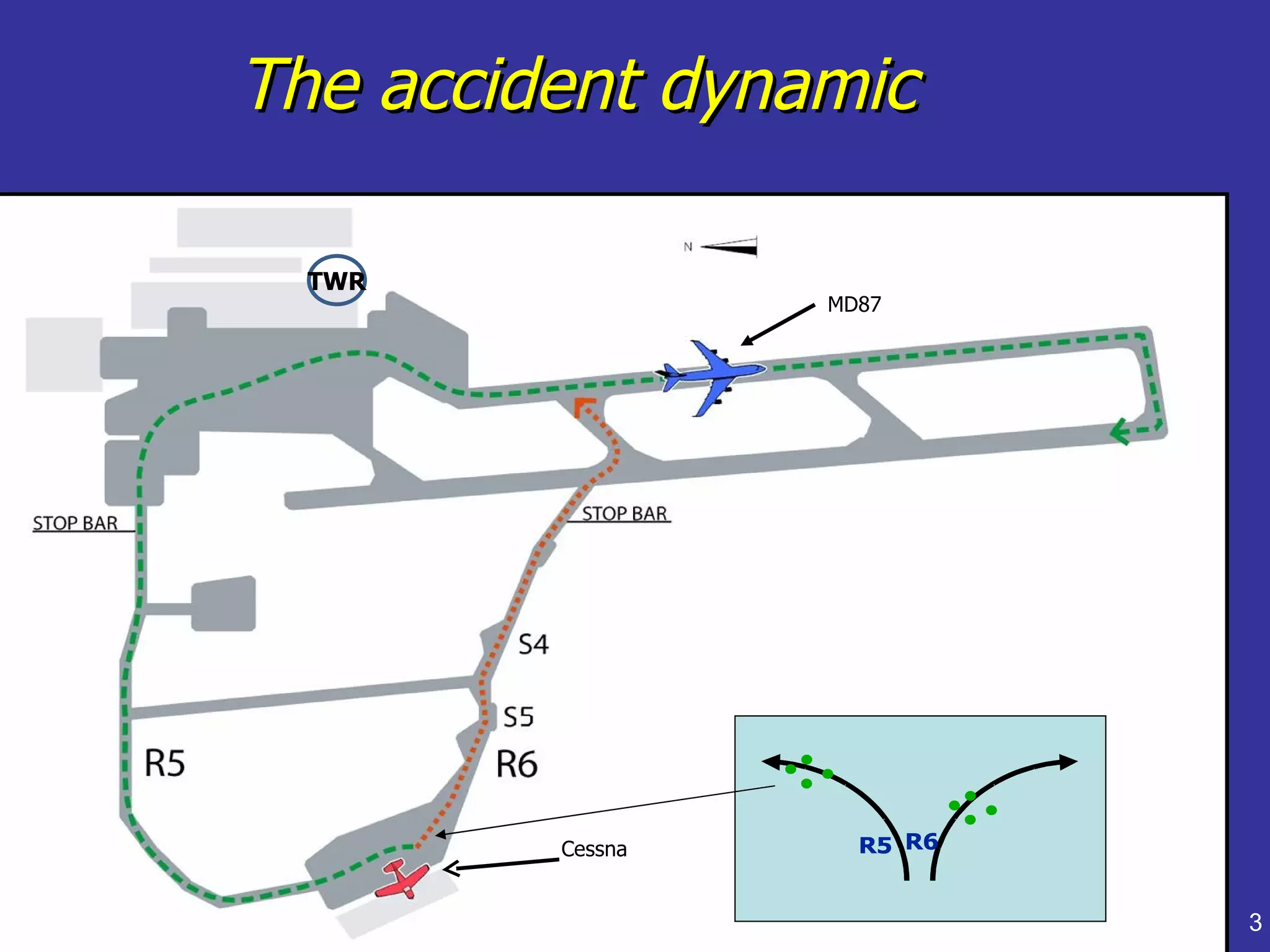
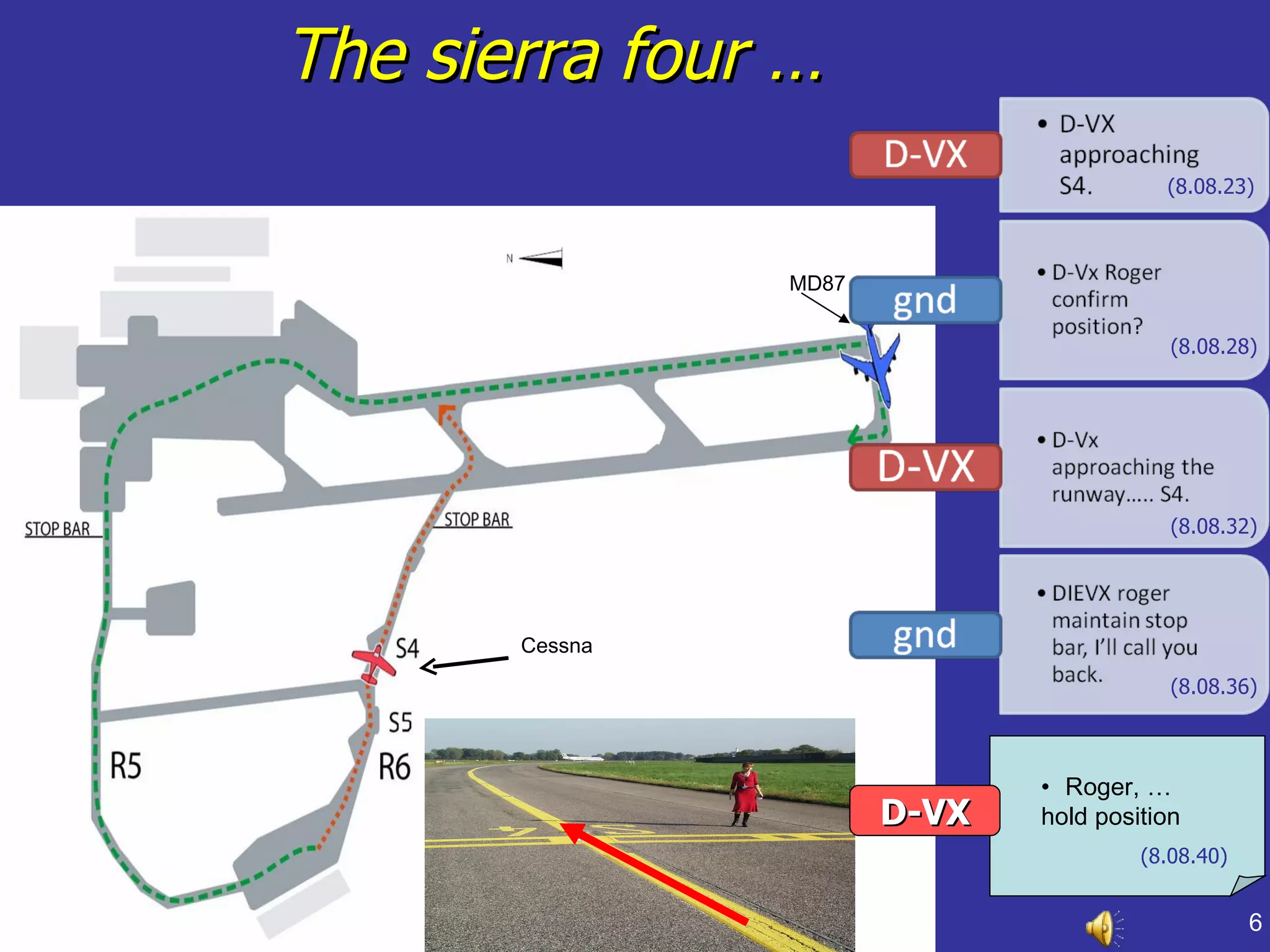
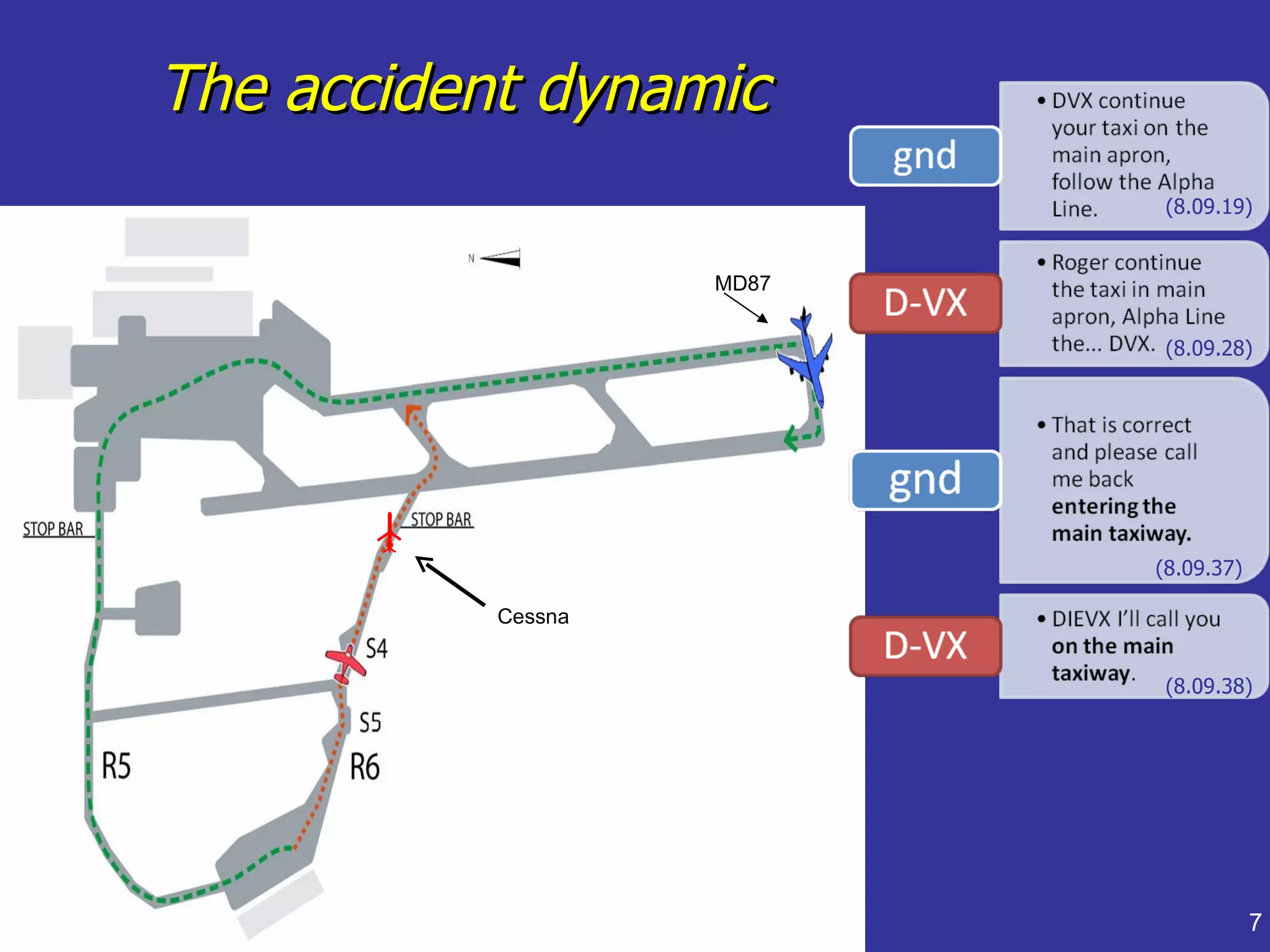
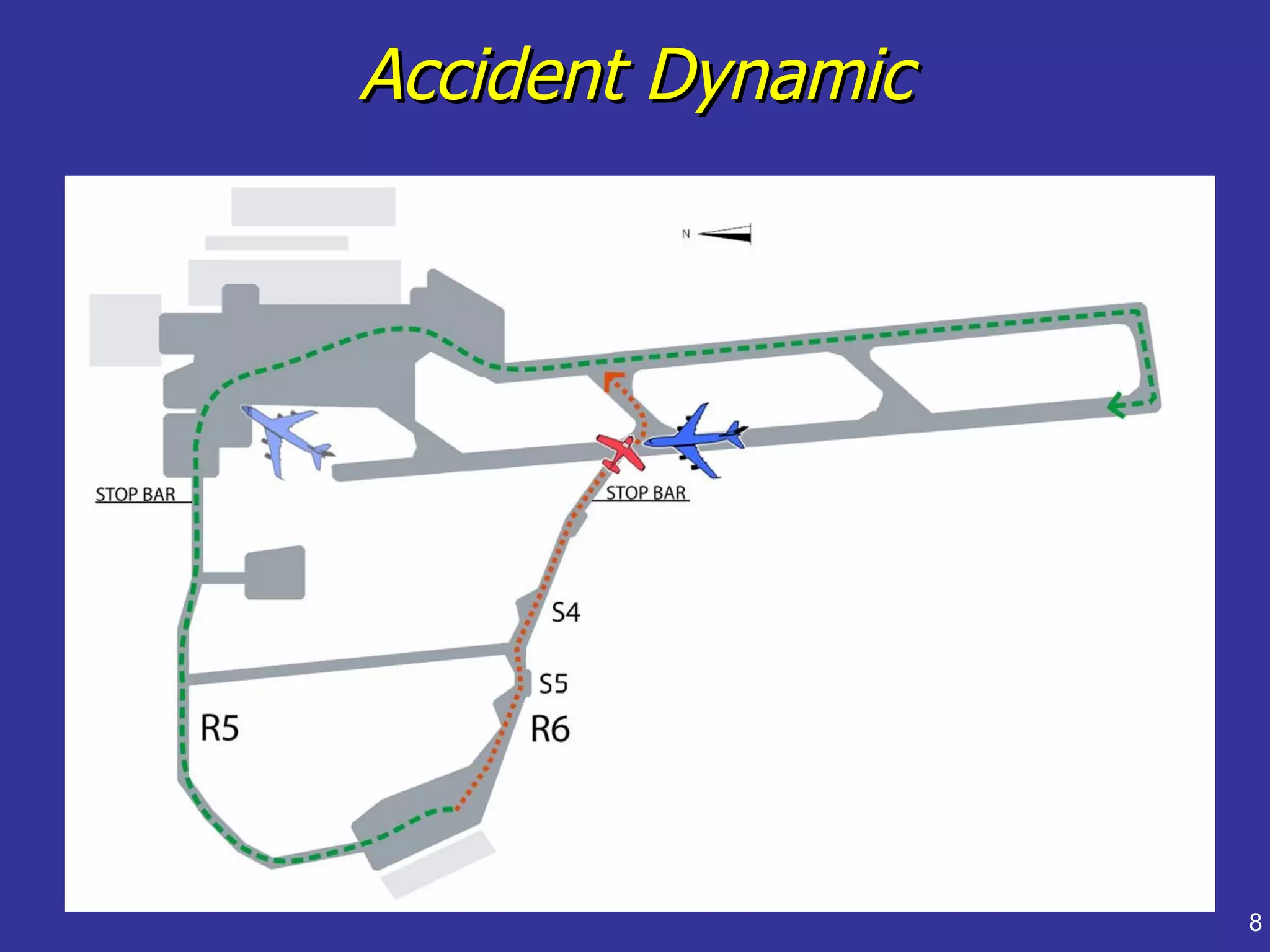
Timeline of events leading to the accident, focusing on dynamics of aircraft interactions.
Identifies key factors including pilot errors, controller mistakes, and negligence contributing to the crash.
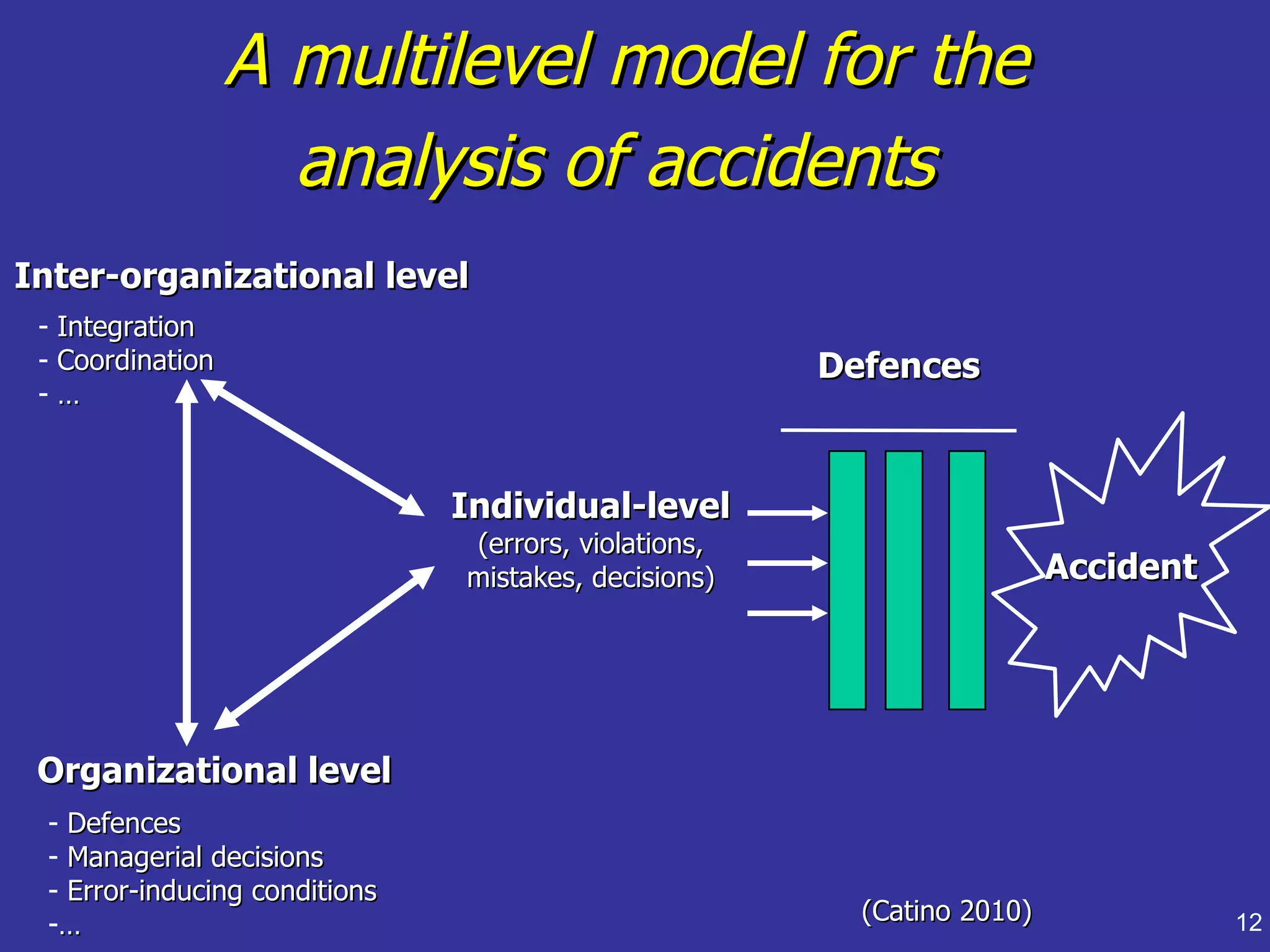
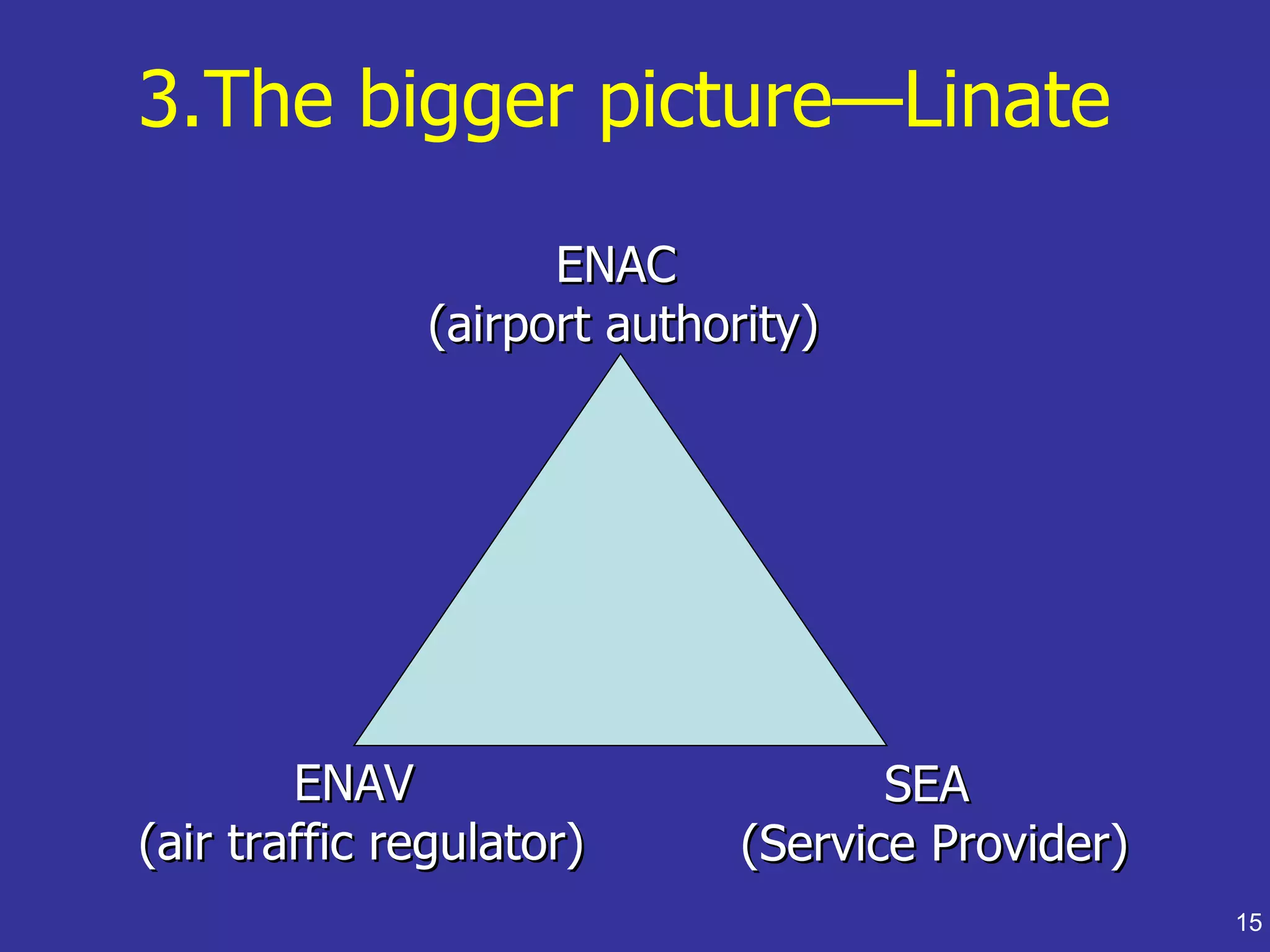
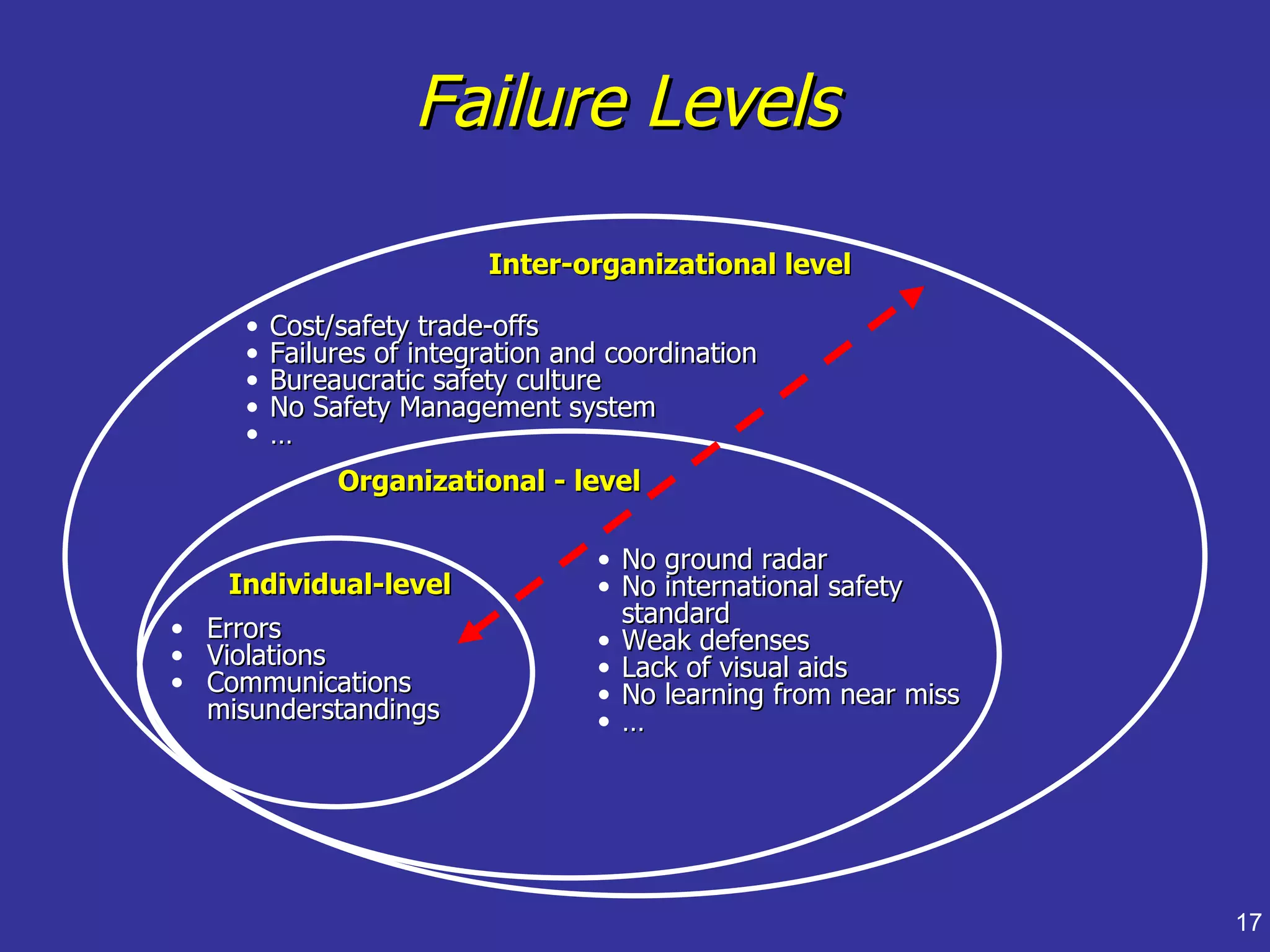
Introduces a model for analyzing accidents across individual, organizational, and inter-organizational levels.
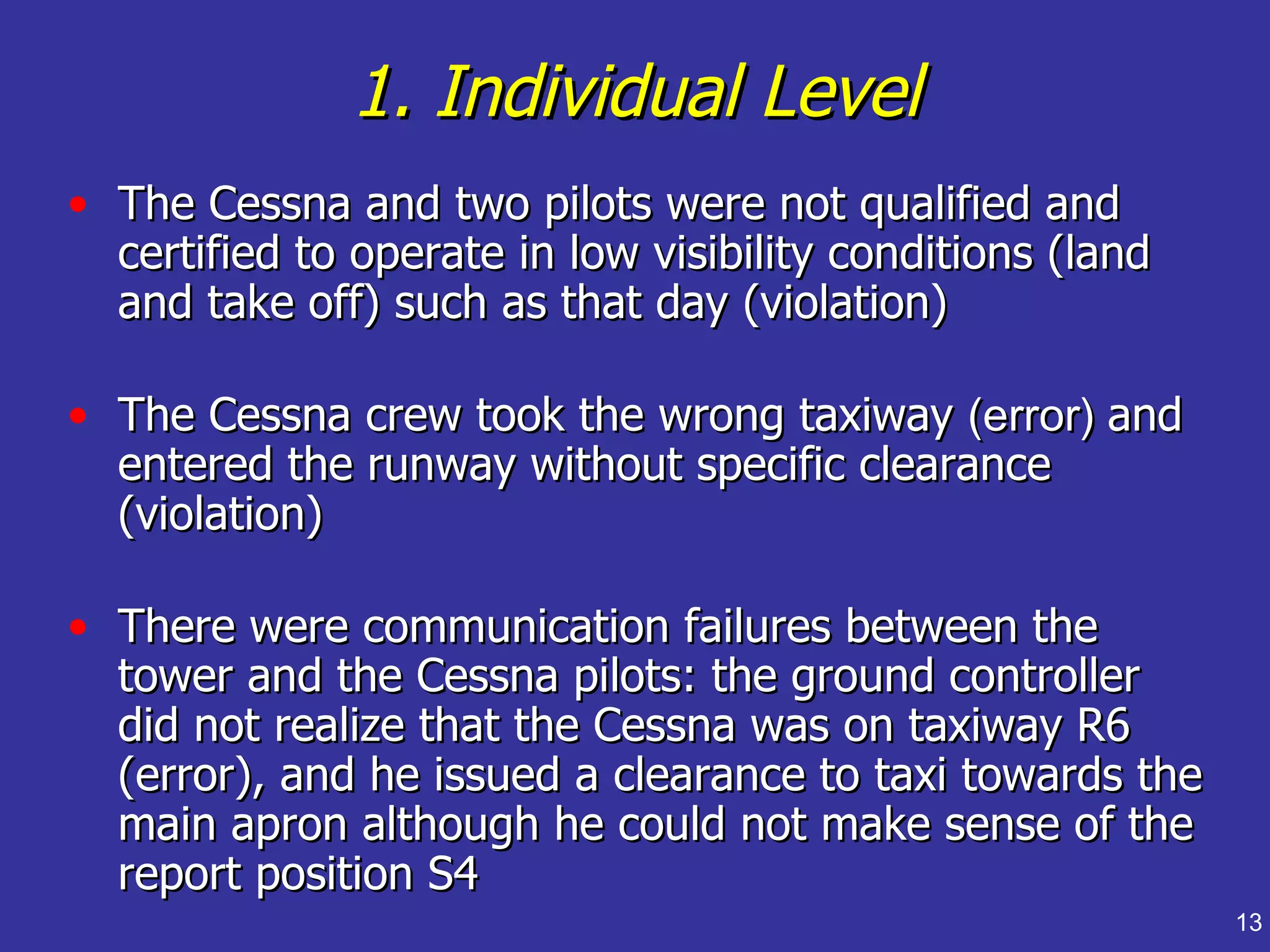
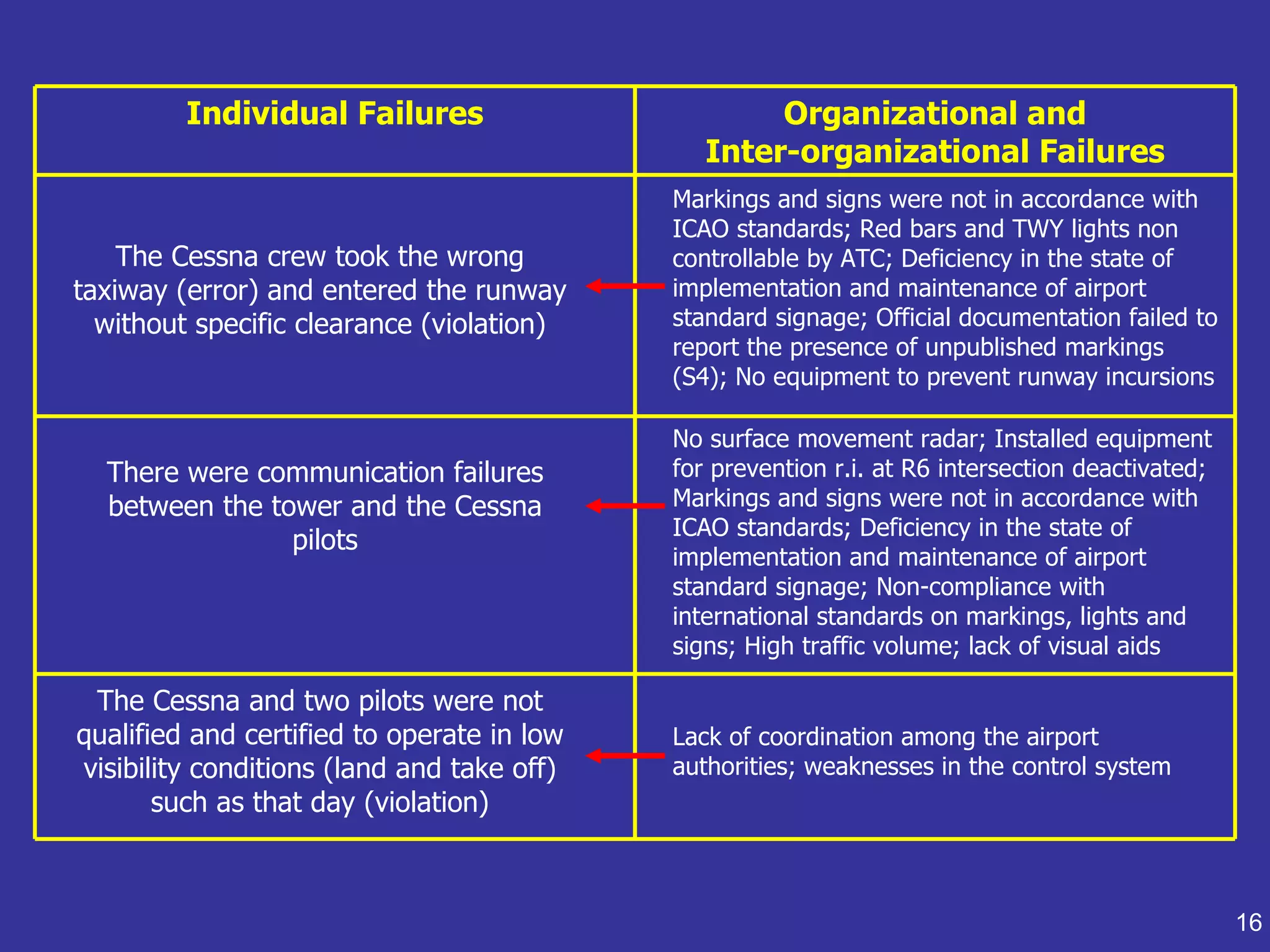
Details specific errors made by Cessna pilots and organizational failures linked to communication and safety.
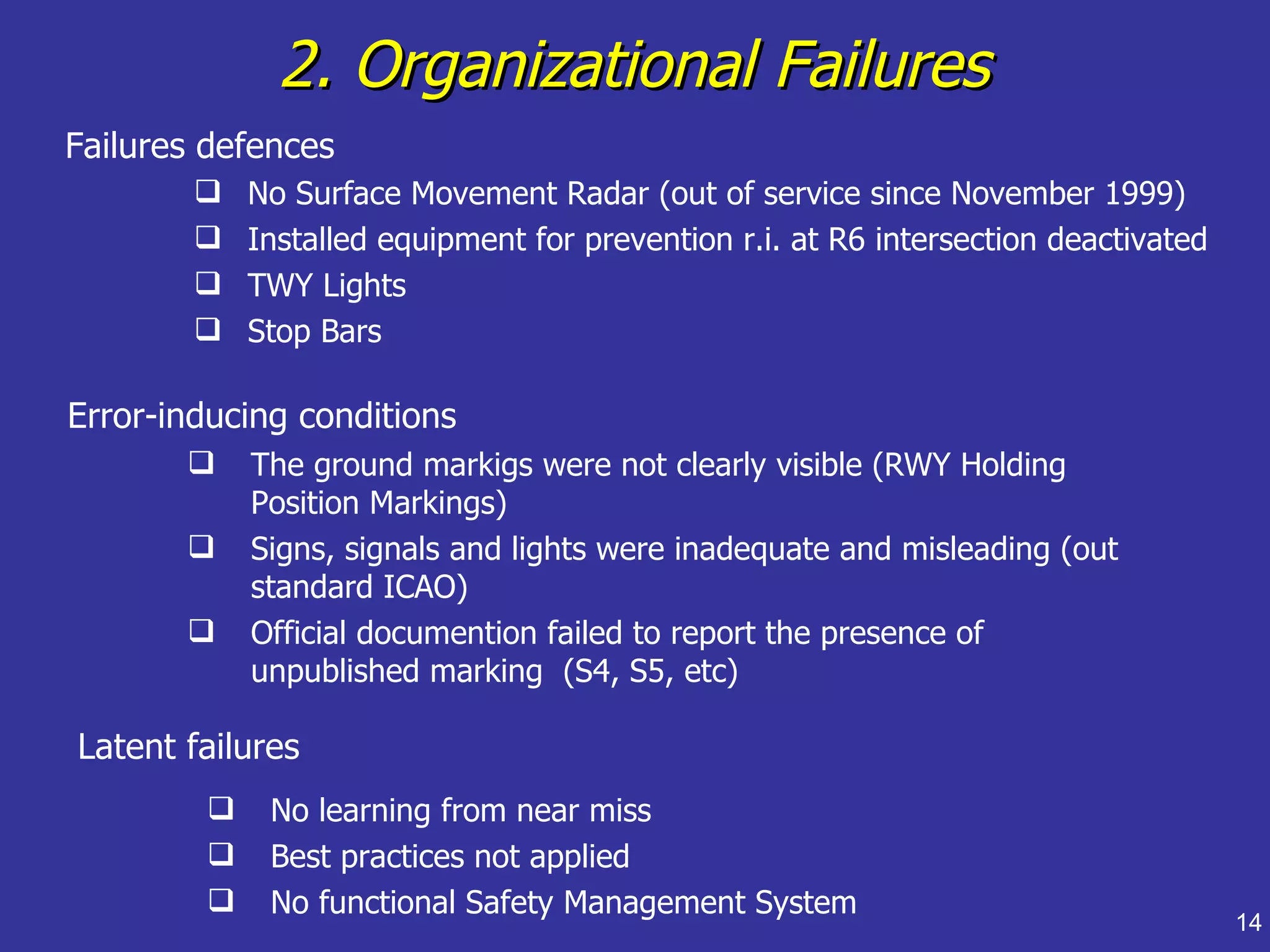
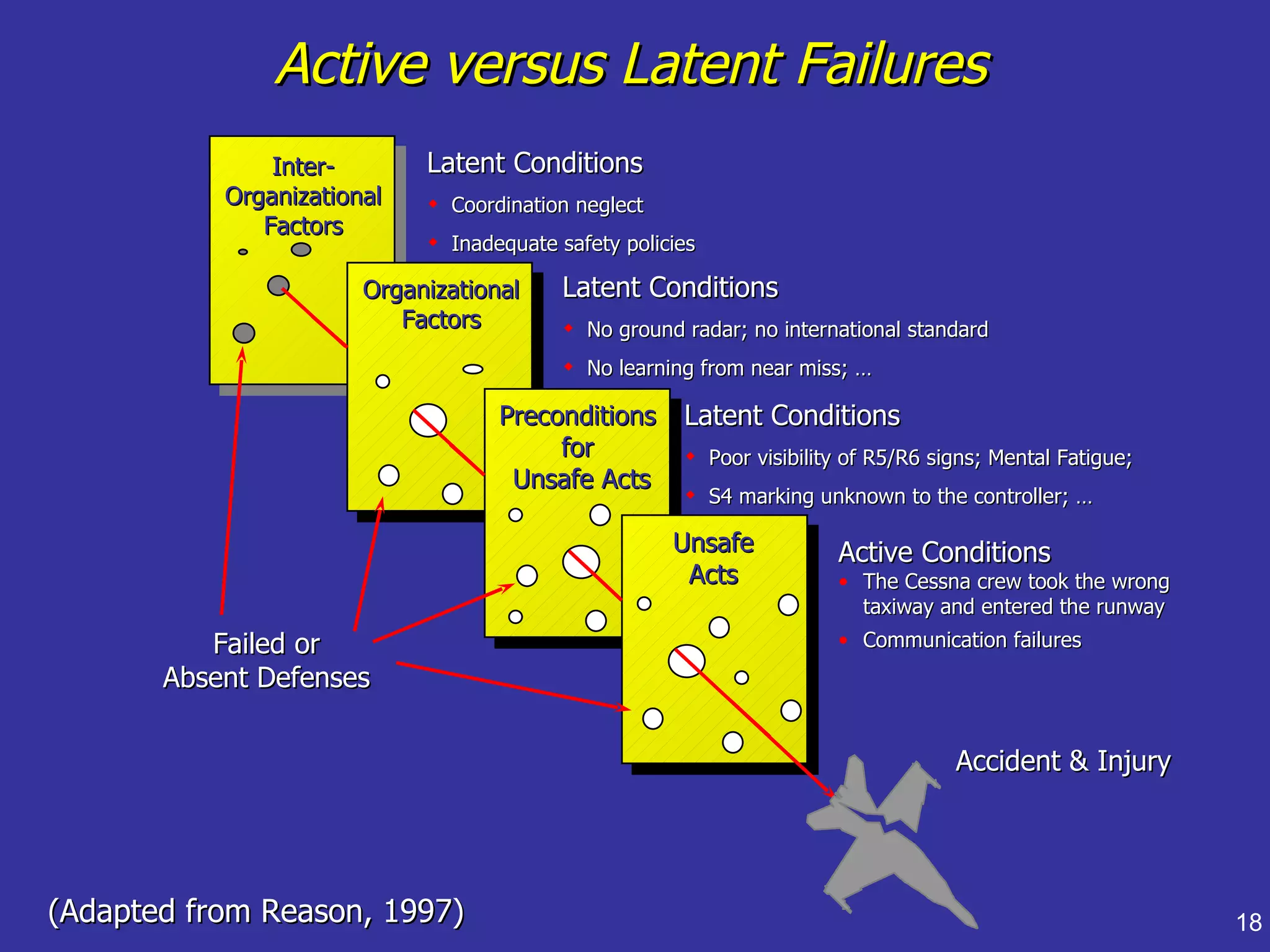
Discusses active vs. latent failures, examining underlying organizational factors leading to the accident.
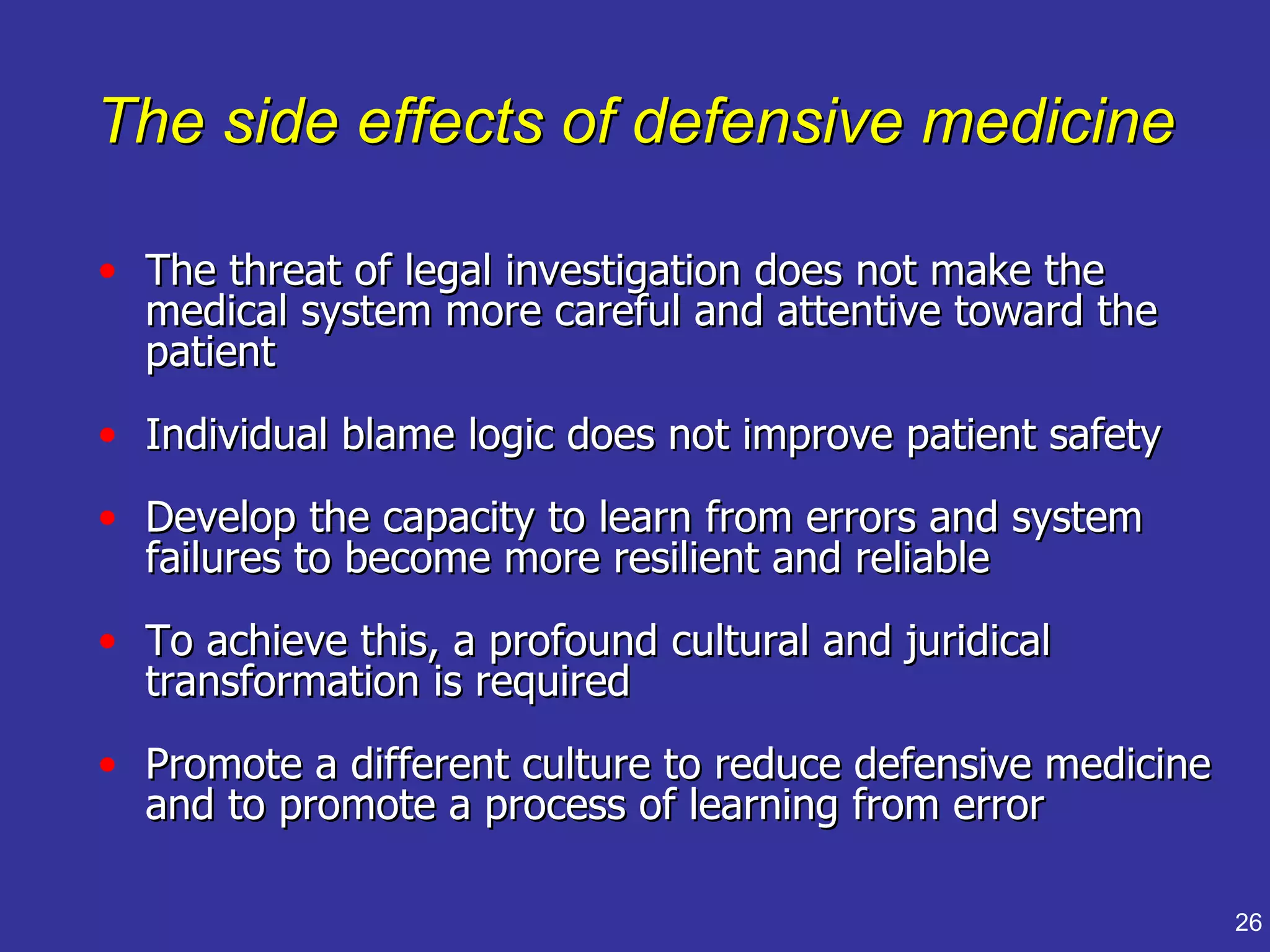
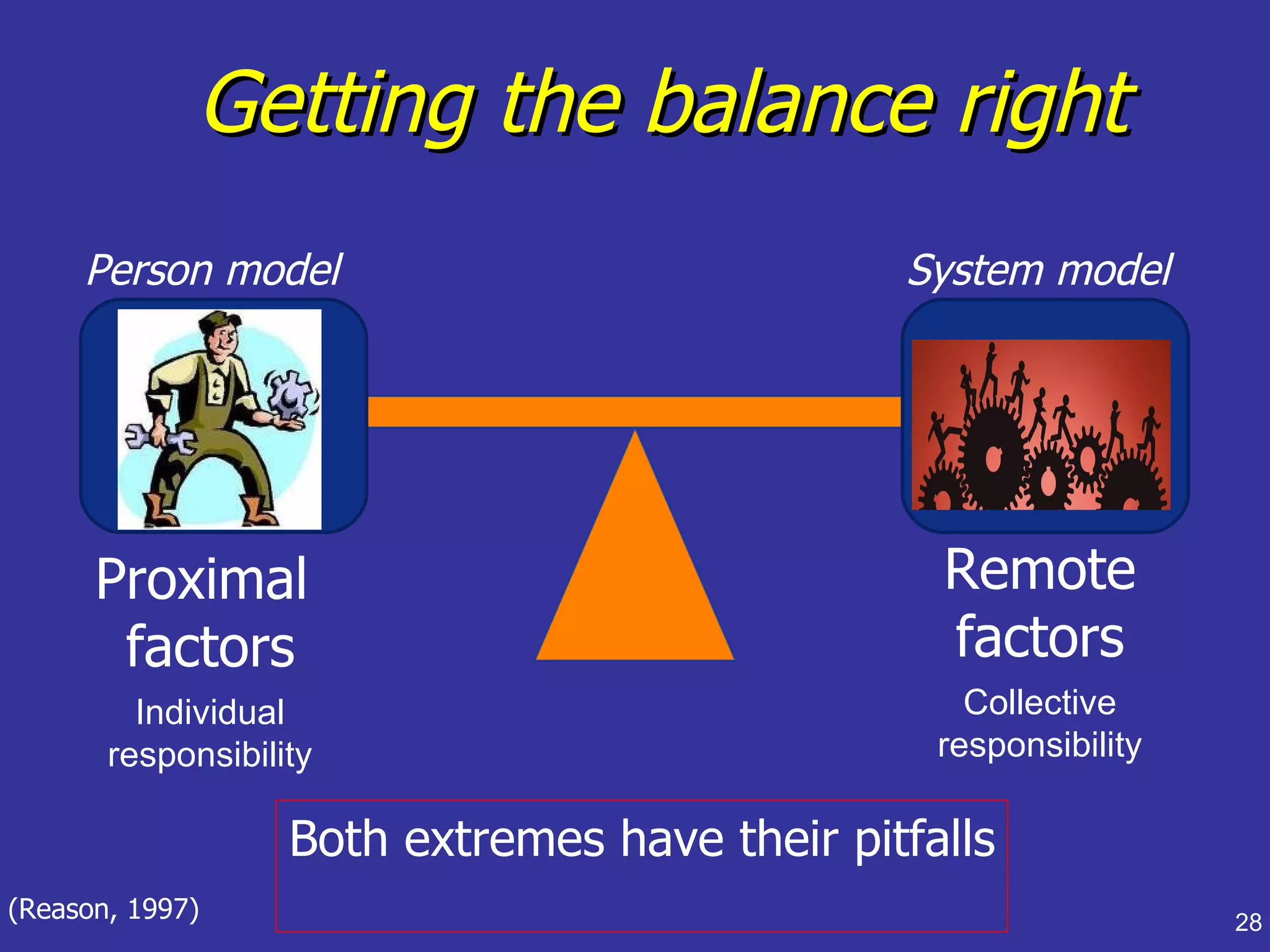
Emphasizes the importance of a system perspective rather than individual blame in analyzing accidents.
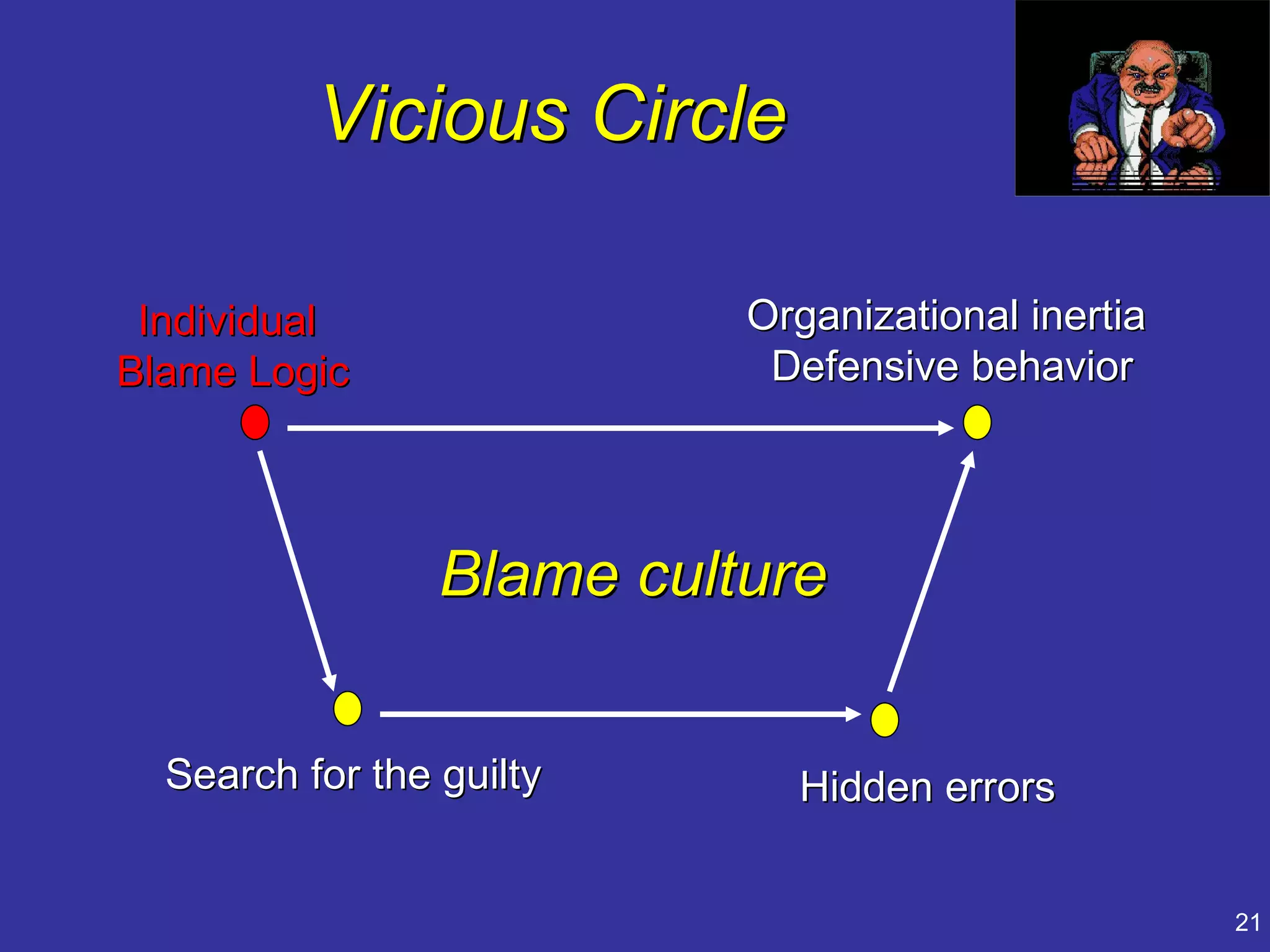
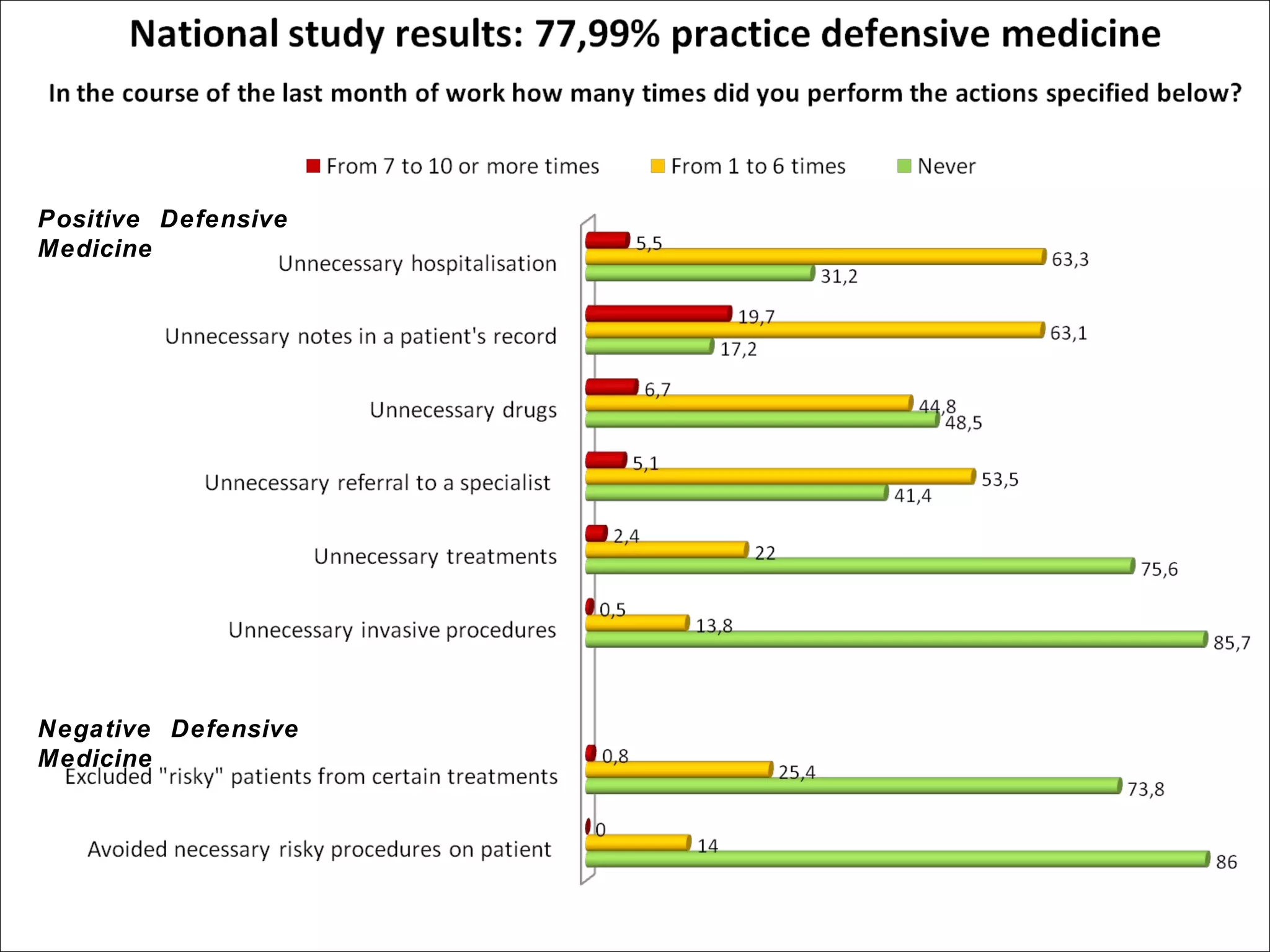
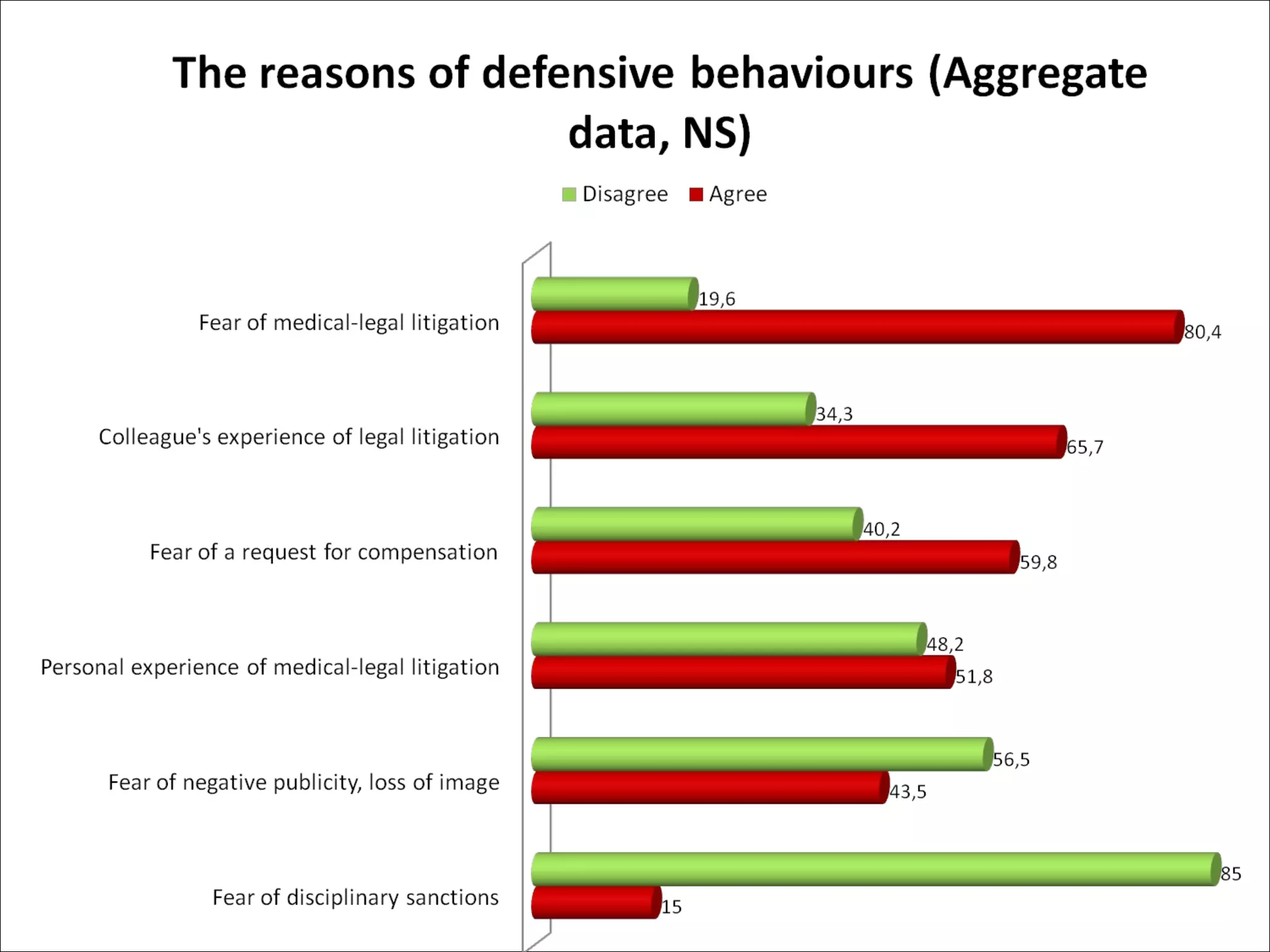
Relates the concept of defensive medicine to organizational errors and the importance of culture in safety.
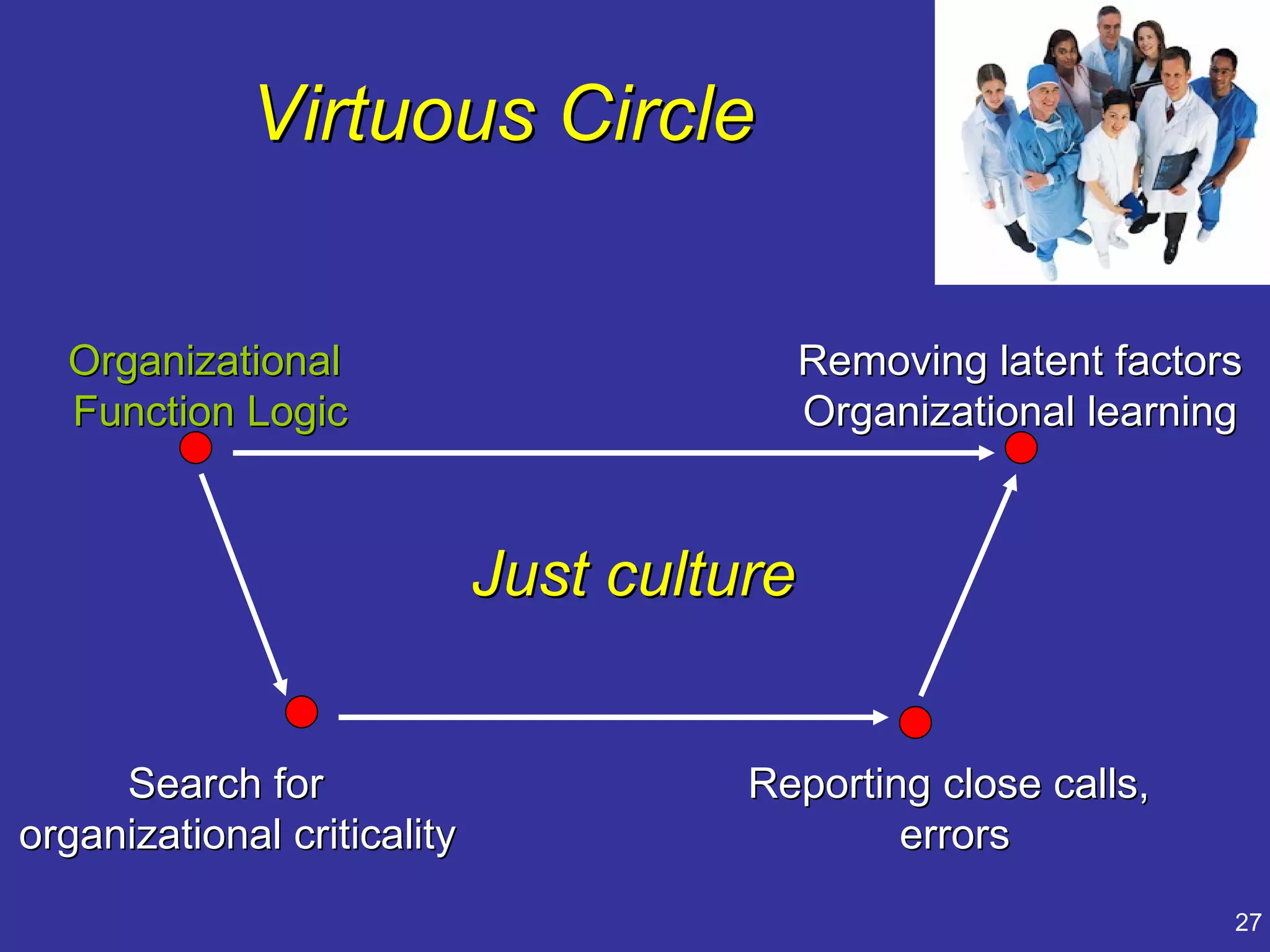
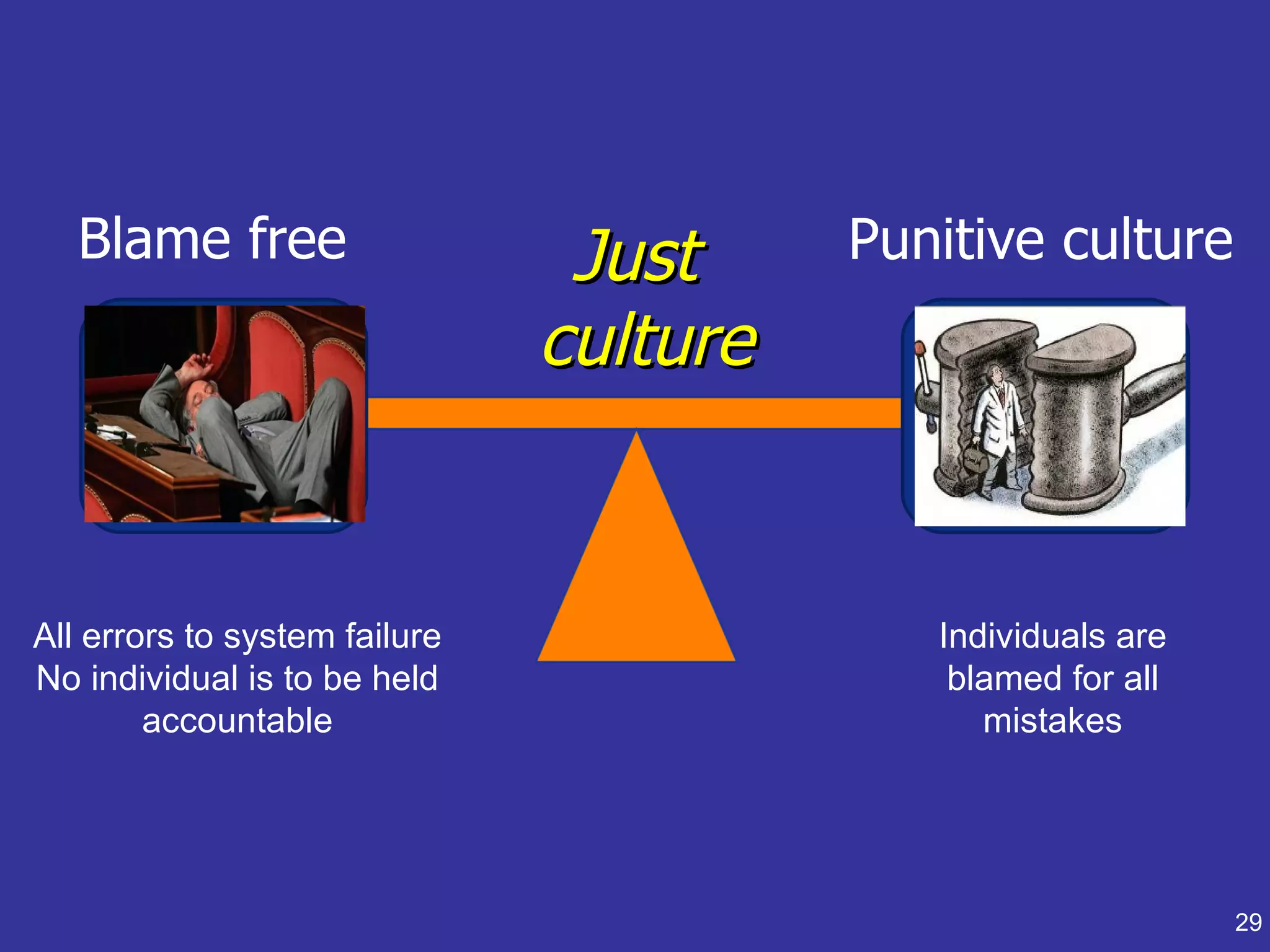
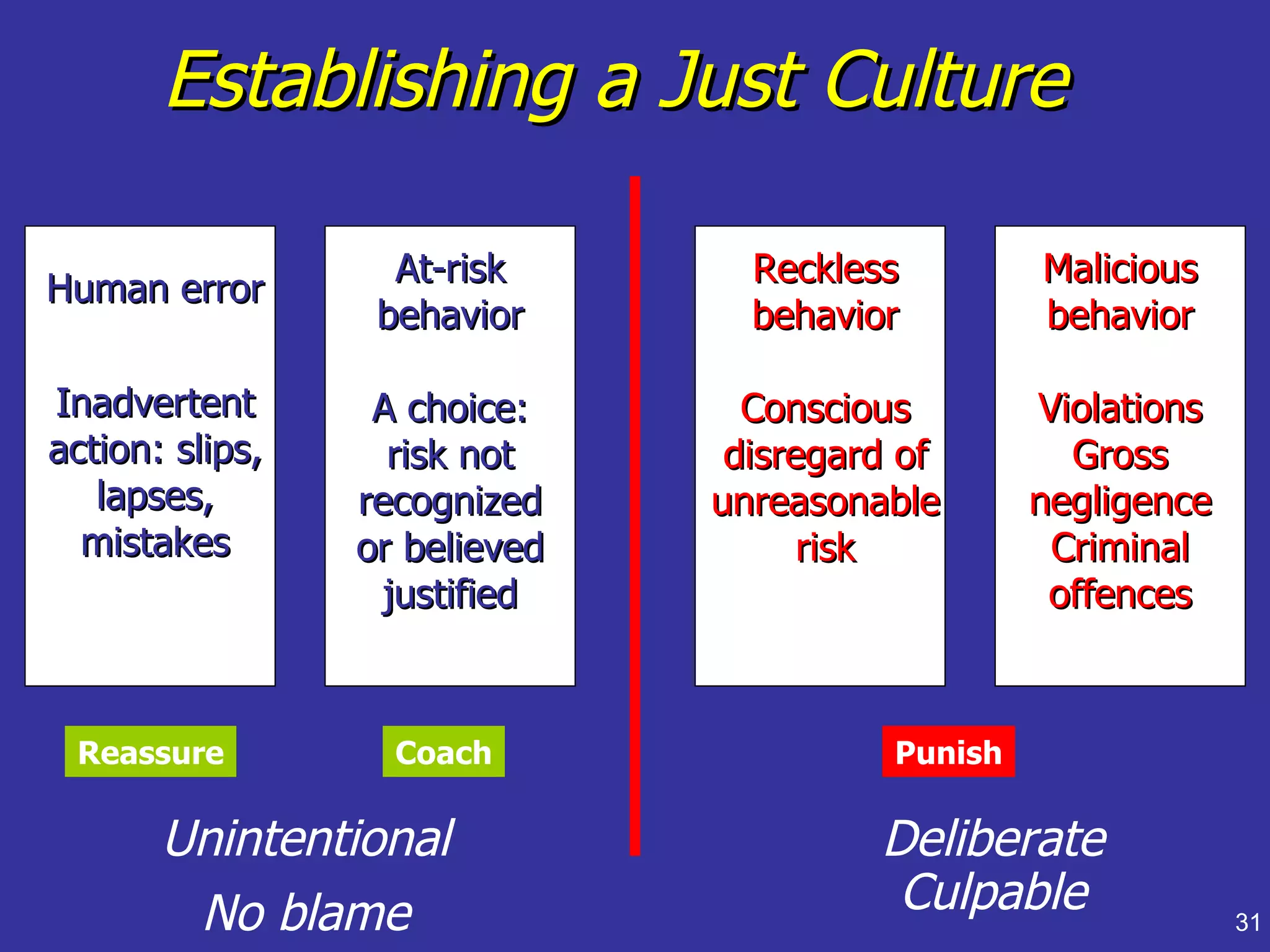
Discusses developing a 'just culture' to improve safety and accountability within organizations.
Examines risk management and safety improvements adopted after incidents in the Italian Air Force.
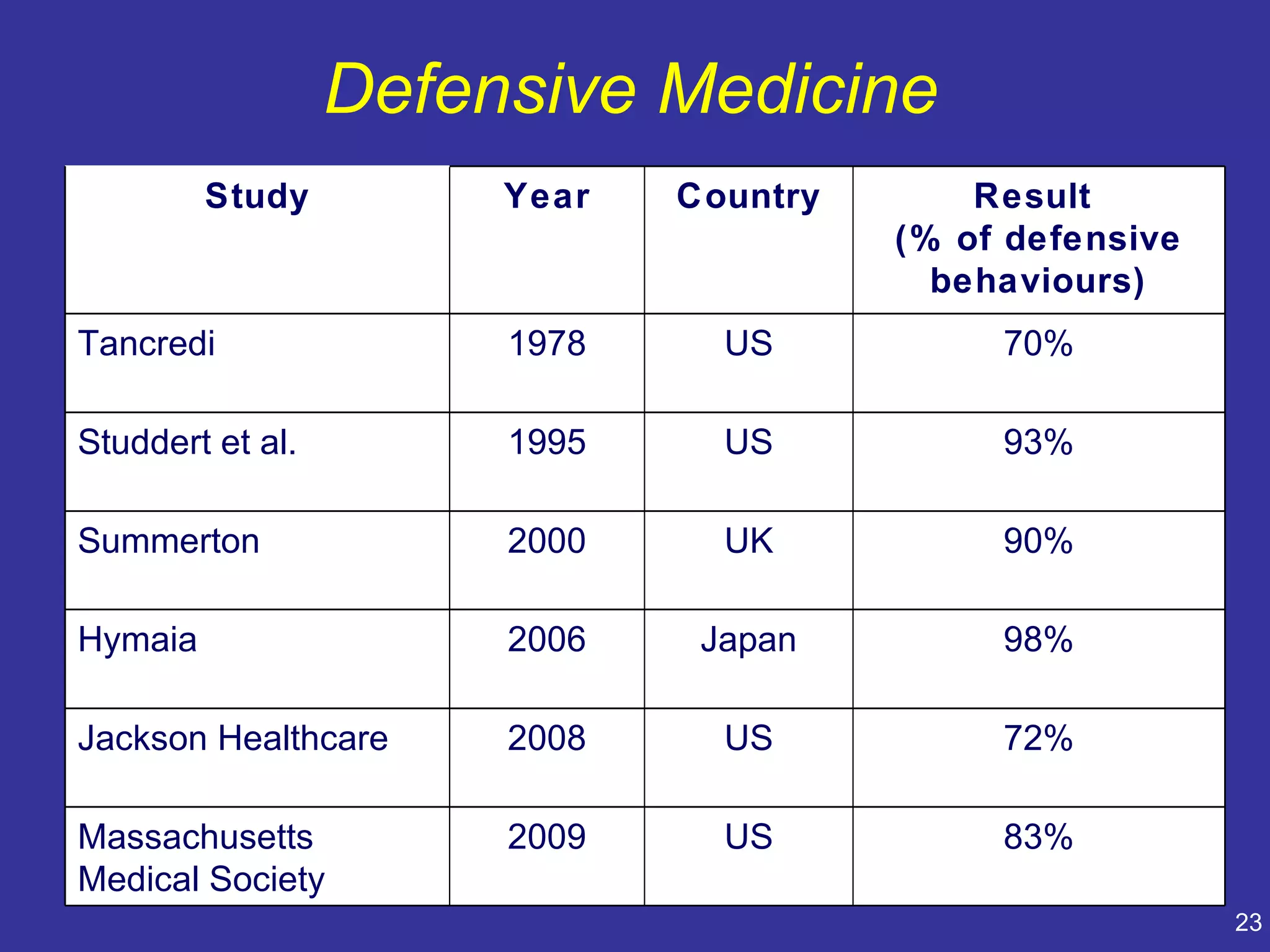
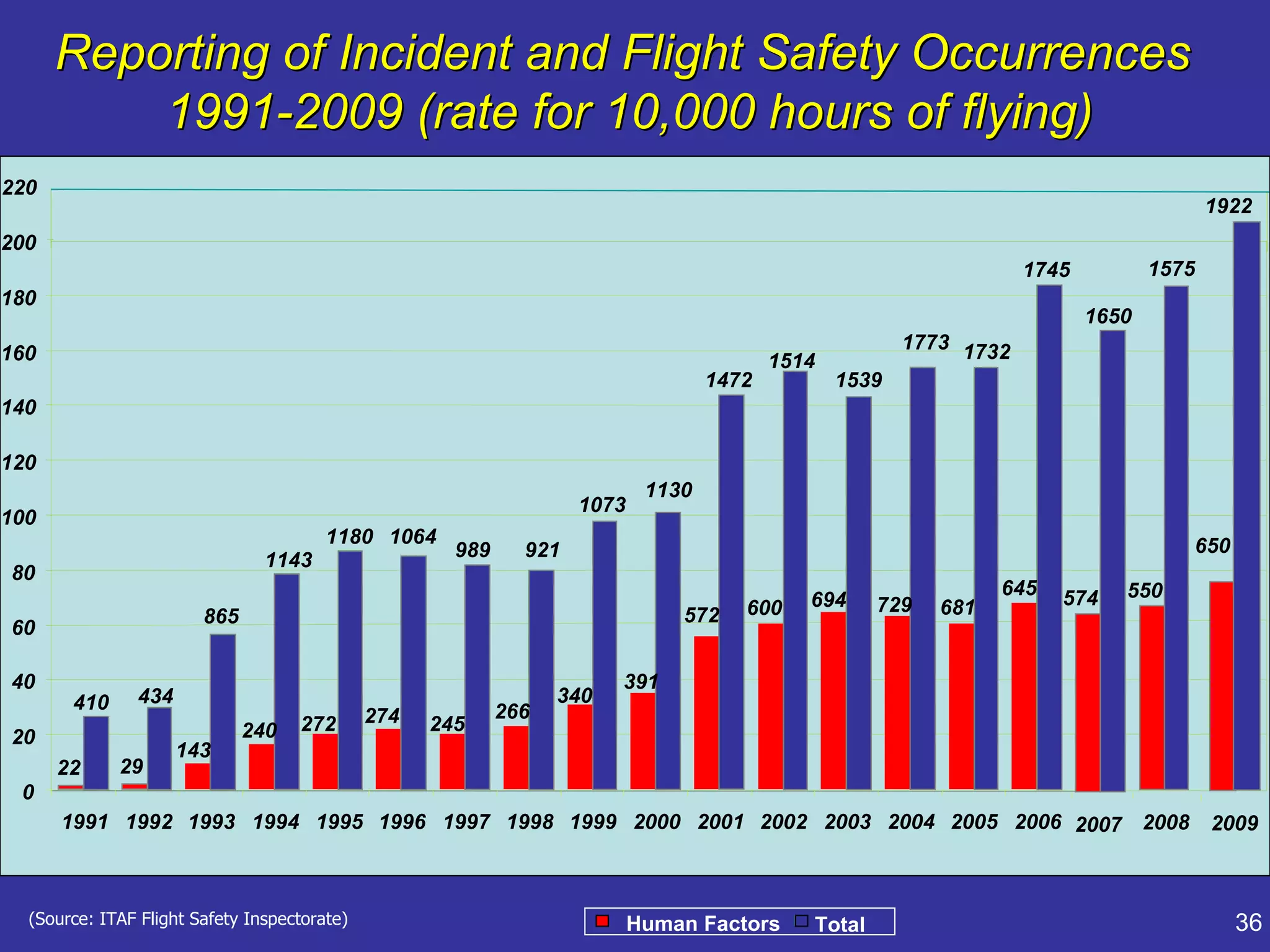
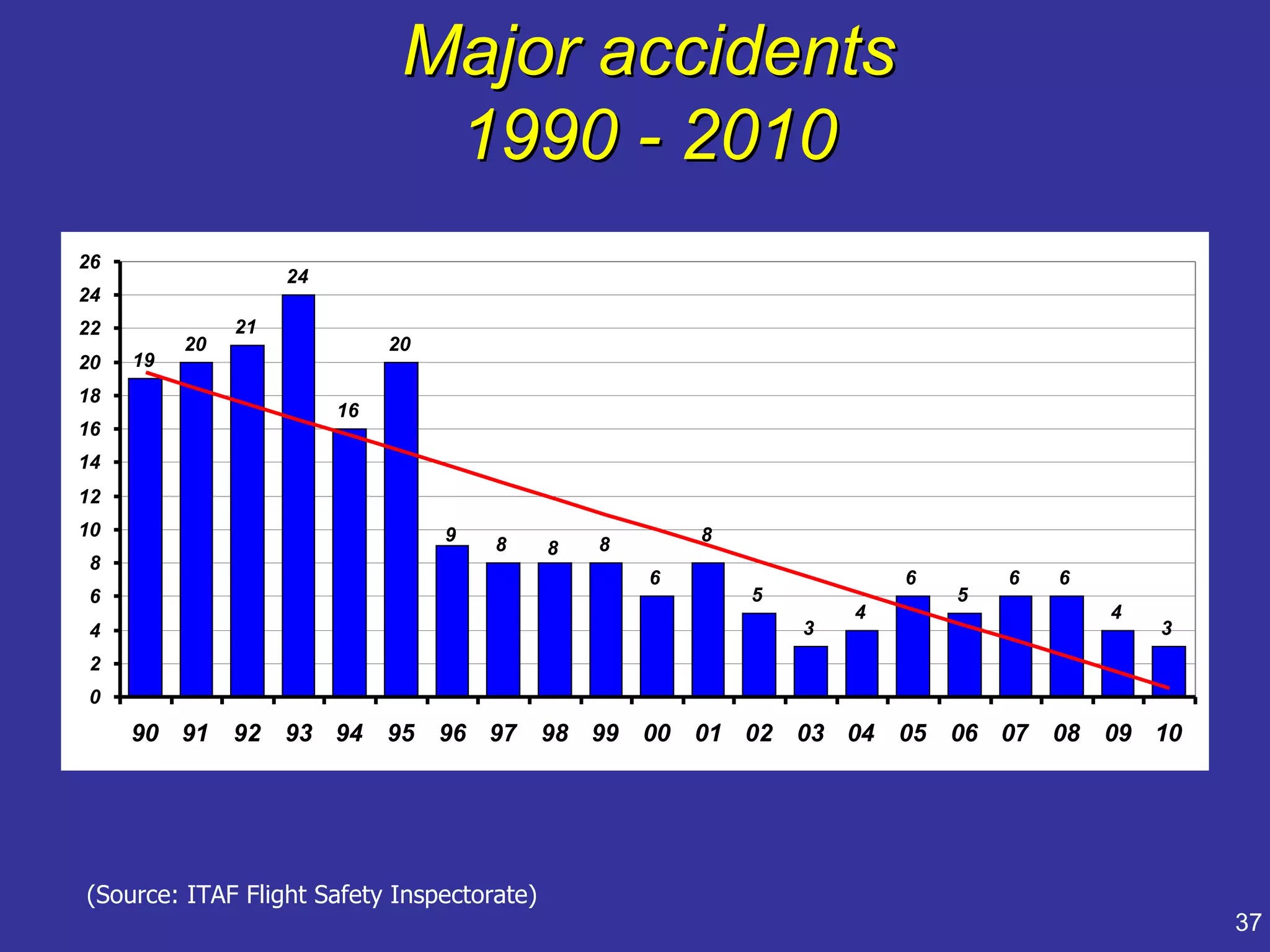
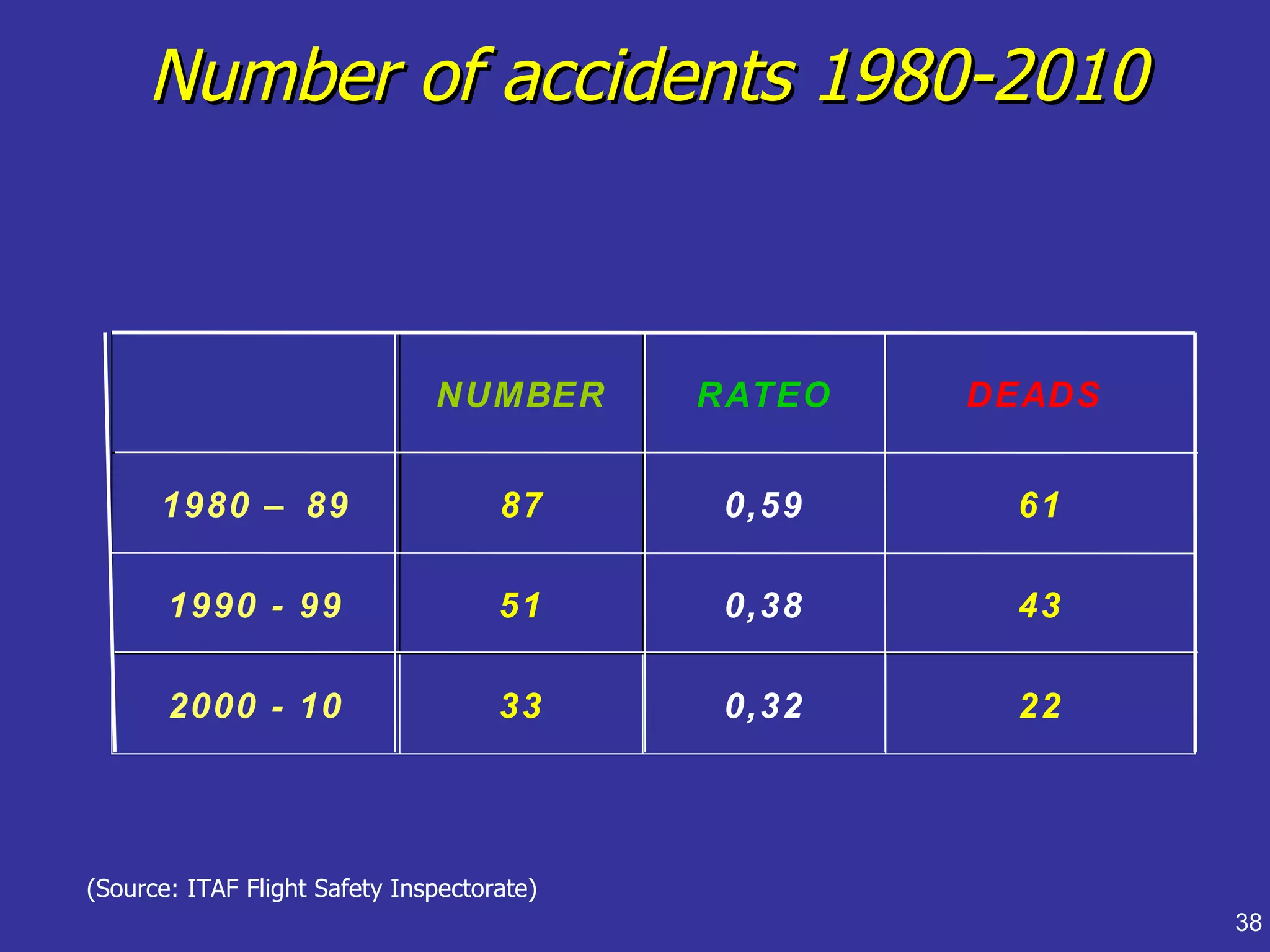
Presents statistical data on accidents and human factors, concluding on managing human error through a just culture.

























































































![[BDD 2025 - Mobile Development] Mobile Engineer and Software Engineer: Are we...](https://cdn.slidesharecdn.com/ss_thumbnails/md-mobileengineerandsoftwareengineerarewestillrelevantsidiqpermana-251127010650-55224ef1-thumbnail.jpg?width=640&height=640&fit=bounds)




![[BDD 2025 - Mobile Development] Crafting Immersive UI with E2E and AGSL Shade...](https://cdn.slidesharecdn.com/ss_thumbnails/md-craftingimmersiveuiwithe2eandagslshaderveronicaputrianggraini-251124030840-0c677f44-thumbnail.jpg?width=640&height=640&fit=bounds)






![[BDD 2025 - Full-Stack Development] PHP in AI Age: The Laravel Way. (Rizqy Hi...](https://cdn.slidesharecdn.com/ss_thumbnails/fs-phpinaiagethelaravelway-251125012602-ef9d330e-thumbnail.jpg?width=640&height=640&fit=bounds)


![[BDD 2025 - Artificial Intelligence] AI for the Underdogs: Innovation for Sma...](https://cdn.slidesharecdn.com/ss_thumbnails/ai-aifortheunderdogsinnovationforsmallbusinesses-251124030839-72a599a4-thumbnail.jpg?width=640&height=640&fit=bounds)


