
Recommended
Recommended
More Related Content
Similar to Psychology in the Schools, Vol. 52(2), 2015 C© 2014 Wiley Peri.docx
Similar to Psychology in the Schools, Vol. 52(2), 2015 C© 2014 Wiley Peri.docx (20)
More from woodruffeloisa
More from woodruffeloisa (20)
Recently uploaded
Recently uploaded (20)
Psychology in the Schools, Vol. 52(2), 2015 C© 2014 Wiley Peri.docx
- 1. Psychology in the Schools, Vol. 52(2), 2015 C© 2014 Wiley Periodicals, Inc. View this article online at wileyonlinelibrary.com/journal/pits DOI: 10.1002/pits.21815 TRAINING TEACHERS TO USE EVIDENCE-BASED PRACTICES FOR AUTISM: EXAMINING PROCEDURAL IMPLEMENTATION FIDELITY AUBYN C. STAHMER AND SARAH RIETH Rady Children’s Hospital, San Diego and University of California, San Diego EMBER LEE Rady Children’s Hospital, San Diego ERICA M. REISINGER AND DAVID S. MANDELL The Children’s Hospital of Philadelphia Center for Autism Research JAMES E. CONNELL AJ Drexel Autism Institute The purpose of this study was to examine the extent to which public school teachers implemented evidence-based interventions for students with autism in the way these practices were designed. Evidence-based practices for students with autism are rarely
- 2. incorporated into community settings, and little is known about the quality of implementation. An indicator of intervention quality is procedural implementation fidelity (the degree to which a treatment is implemented as prescribed). Procedural fidelity likely affects student outcomes. This project examined procedural implemen- tation fidelity of three evidence-based practices used in a randomized trial of a comprehensive program for students with autism in partnership with a large, urban school district. Results indicate that teachers in public school special education classrooms can learn to implement evidence-based strategies; however, they require extensive training, coaching, and time to reach and maintain moderate procedural implementation fidelity. Procedural fidelity over time and across intervention strategies is examined. C© 2014 Wiley Periodicals, Inc. Special education enrollment for children with autism in the United States has quadrupled since 2000 (Scull & Winkler, 2011), and schools struggle to provide adequate programming to these students. A growing number of interventions for children with autism have been proven efficacious in university-based research settings, but much less attention has been given to practical issues of implementing these programs in the classroom, where most children with autism receive the majority of their care (Sindelar, Brownell, & Billingsley, 2010). In general, evidence-based practices for children with autism are rarely incorporated into community settings (Stahmer & Ingersoll, 2004). Teachers in public schools report receiving inadequate training and rate their personal efficacy in working with children with autism as low (Jennett, Harris, &
- 3. Mesibov, 2003). Training public educators to provide evidence-based practices to children with autism is a central issue facing the field (Simpson, de Boer-Ott, & Smith-Myles, 2003). One major challenge to implementing evidence-based practices for children with autism in community settings is the complexity of these practices. Strategies based on the principles of applied behavior analysis have the strongest evidence to support their use (National Standards This research was funded by grants from the National Institute of Mental Health (5R01MH083717) and the Institute of Education Sciences (R324A080195). We thank the School District of Philadelphia and its teachers and families for their collaboration and support. Additionally, Dr. Stahmer is an investigator with the Implementation Research Institute at the George Warren Brown School of Social Work, Washington University, St. Louis, through an award from the National Institute of Mental Health (R25MH080916). Correspondence to: Aubyn C. Stahmer, Child and Adolescent Services Research Center & Autism Discovery Institute, Rady Children’s Hospital, San Diego, 3020 Children’s Way, MC5033, San Diego, CA 92123. E-mail: [email protected] 181 182 Stahmer et al. Project, 2009). These practices vary greatly in structure and difficulty. Some strategies, such as
- 4. discrete trial teaching (DTT; Leaf & McEachin, 1999; Lovaas, 1987), are highly structured and occur in one-on-one settings, whereas others are naturalistic, can be conducted individually or during daily activities, and tend to be more complex to implement (e.g., incidental teaching; Fenske, Krantz, & McClannahan, 2001; or pivotal response training [PRT]; Koegel et al., 1989). There are also classroom-wide strategies and structures based on applied behavior analysis, such as teaching within functional routines (FR; Brown, Evans, Weed, & Owen, 1987; Cooper, Heron, & Heward, 1987; Marcus, Schopler, & Lord, 2000; McClannahan & Krantz, 1999). Although all of these evidence- based practices share the common foundational principles of applied behavior analysis, each is made up of different techniques. These and other intervention techniques are often packaged together as “comprehensive interventions” (Odom, Boyd, Hall, & Hume, 2010) or used in combination in the field to facilitate learning and expand the conditions under which new student behaviors occur (Hess, Morrier, Heflin, & Ivey, 2008; Stahmer, 2007). Teachers can learn these evidence-based strategies within the context of a research study (e.g., Suhrheinrich, 2011); however, studies report a highly variable number of hours of training needed to master the intervention strategy. For example, the amount of time required to train classroom educators in DTT in published studies ranges from 3 hours (Sarokoff & Sturmey, 2004) at its most brief, to recommendations of 26 to 60 hours of supervised experience (Koegel, Russo, & Rincover, 1977; Smith, Buch, & Gamby, 2000; Smith, Parker, Taubman, & Lovaas, 1992). Teachers have been
- 5. trained to fidelity in PRT in 8 to 20 hours (Suhrheinrich, 2011). To achieve concurrent mastery of several different intervention techniques and to incorporate the development of appropriate student goals, some researchers have suggested that teachers may need a year or more of full-time, supervised practicum training (Smith, Donahoe, & Davis, 2000). There are several reasons why teachers may not implement evidence-based practices the way they were designed. First, teachers typically receive limited instruction in specific interventions. For example, instruction often comprises attendance at a didactic workshop and receipt of a manual. Teachers are then expected to implement evidence-based practices without the ongoing coaching and feedback that is critical for intervention mastery (Bush, 1984; Cornett & Knight, 2009). Second, most evidence-based practices were not designed for school settings and therefore may be difficult to implement appropriately in the classroom (Stahmer, Suhrheinrich, Reed, Bolduc, & Schreibman, 2011). Perhaps as a result, teachers often report that they combine or modify evidence-based practices to meet the specific needs of their classroom and students (Stahmer, Collings, & Palinkas, 2005). Finally, school administrators sometimes mandate the use of programs that may not align with teachers’ classroom environment, beliefs, or pedagogy (Dingfelder & Mandell, 2011). A major indication of the quality of the implementation of any evidence-based practices is treatment fidelity, also known as implementation fidelity (Gersten et al., 2005; Horner et al., 2005; Noell, Duhon, Gatti, & Connell, 2002; Noell et al., 2005;
- 6. Proctor et al., 2011; Schoenwald et al., 2011). Implementation fidelity is the degree to which a treatment is implemented as prescribed, or the level of adherence to the specific procedures of the intervention (e.g., Gresham, 1989; Rabin, Brownson, Haire-Joshu, Kreuter, & Weaver, 2008; Schoenwald et al., 2011). There are several types of implementation fidelity. Procedural fidelity (Odom et al., 2010; also called program adherence; Schoenwald et al., 2011) is the degree to which the provider uses procedures required to execute the treatment as intended. Other types of fidelity include treatment differentiation (the extent to which treatments differ from one another), therapist competence (the level of skill and judgment used in executing the treatment; Schoenwald et al., 2011), and dosage (Odom et al., 2010). Although, ideally, all types of fidelity would be examined to determine the fit of an intervention in a school program (Harn, Parisi, & Stoolmiller, 2013), procedural fidelity provides one important avenue for Psychology in the Schools DOI: 10.1002/pits Training Teachers in Autism Practices 183 measuring the extent to which an intervention resembles an evidence-based practice or elements of evidence-based practice (Garland, Bickman, & Chorpita, 2010). Procedural implementation fidelity is likely a potential mediating variable affecting student outcomes, with higher fidelity resulting in better outcomes (Durlak & DuPre, 2008; Gresham,
- 7. MacMilan, Beebe-Grankenberger, & Bocian, 2000; Stahmer & Gist, 2001); however, it is not often measured. In behavioral services research, three separate reviews of reported implementation fidelity data have been published. In the Journal of Applied Behavior Analysis, fidelity data were reported in only 16% to 30% of published articles (Gresham, Gansle, & Noell, 1993; McIntyre, Gresham, DiGennaro, & Reed, 2007; Peterson, Homer, & Wonderlich, 1982). Three separate reviews indicated that only 13% to 32% of autism intervention studies included fidelity measures (Odom & Wolery, 2003; Wheeler, Baggett, Fox, & Blevins, 2006; Wolery & Garfinkle, 2002). A recent review of special education journals found that fewer than half (47%) of intervention articles reported any type of fidelity scores (Swanson, Wanzek, Haring, Ciullo, & McCulley, 2011). Indeed, limited reporting of implementation adherence is evident across a diverse body of fields (Gresham, 2009). The lack of reporting (and therefore, the presumable lack of actual measurement of implementation) limits the conclusions that can be drawn regarding the association between student outcomes and the specific treatment provided. Therefore, examination of implementation fidelity, although complicated, is important to advance the understanding of how evidence-based interventions are being implemented in school settings. Our research team recently completed a large-scale randomized trial of a comprehensive pro- gram for students with autism in partnership with a large, urban public school district. Procedural implementation fidelity of the overall program (which includes three evidence-based practices) was
- 8. highly variable, ranging from 12% to 92% (Mandell et al., 2013). The three strategies included in this program, DTT, PRT, and FR (see description in the Method section), share an underlying theo- retical base, but rely on different specific techniques. The purpose of this study was to examine the extent to which public school teachers implemented evidence- based interventions for students with autism in the way these practices were designed. Examining implementation fidelity of each strategy individually may provide insight into whether specific interventions are more easily implemented in the classroom environment. In particular, we examined whether special education classroom teach- ers and staff: 1) mastered specific strategies that form the backbone of applied behavioral analysis programs for autism; 2) used the strategies in their classroom; and 3) maintained their procedural fidelity to these strategies over time. METHOD Participants Participants were classroom teachers and staff in an urban school district’s kindergarten- through-second-grade autism support classrooms (each in a different school) participating in a larger trial of autism services. Of the 67 total autism support classrooms in the district at the time of the study, teachers and staff from 57 (85%) of the schools participated. Each classroom included one participating teacher and 0 to 2 classroom assistants (M = 1). Throughout the district, staff were required to participate in intervention training as part of professional development, but were not
- 9. required to consent to participate in the study. Data from the current study are reported only for the 57 teachers and staff who consented to participate. Teachers received intensive training in Strategies in Teaching Based on Autism Research (STAR) during their first year of participation in the project. During the second year, continuing teachers received in-classroom coaching every other week. From the original 57, 38 teachers (67%) Psychology in the Schools DOI: 10.1002/pits 184 Stahmer et al. Table 1 Teacher Demographic Characteristics N % Female Total Years Teaching, M (range) Years Teaching Children with ASD, M (range) Education Level % Bachelor’s Degree/% Master’s Degree
- 10. 57 97.3 10.8 (1–38) 6.8 (1–33) 30/70 participated in the second year of the study. See Table 1 for teacher demographics. A complete description of adult and student participants can be found elsewhere (Mandell et al., 2013). Intervention Strategies for Teaching Based on Autism Research. The goal of the Strategies for Teaching Based on Autism Research (STAR) program is to develop children’s skills in a highly structured environment and then generalize those skills to more naturalistic settings. The program includes a curriculum in which each skill is matched to a specific instructional strategy. The STAR program includes three evidence-based strategies: DTT, PRT, and FR. DTT relies on highly structured, teacher-directed, one-on-one interactions between the teacher and student. In these interactions, the teacher initiates a specific stimulus to evoke the child’s response, generally a discrete skill, which is an element of a larger behavioral repertoire (Krug et al., 1979; Krug, Rosenblum, Almond, & Arick, 1981; Lovaas, 1981, 1987; Smith, 2001). DTT is used in STAR for teaching pre-academic and receptive language skills, where the desired behavior takes a very specific form, such as learning to identify colors, sequencing events from a story into a first-next-then-last structure or counting with one-to-one correspondence. The consequence of the desired behavior is an external reinforcer, such as a token or a preferred edible (Lovaas, 2003; Lovaas
- 11. & Buch, 1997). PRT can occur in both one-on-one interactions and small-group interactions with the teacher. It is considered student directed because it occurs in the regular classroom environment, where the teaching area is pre-arranged to include highly preferred activities or toys that the student will be motivated to acquire. In PRT, students initiate the teaching episode by indicating interest in an item or activity or selecting among available teaching materials. Materials are varied frequently to enhance student motivation and generalization of skills and make PRT appropriate for targeting expressive and spontaneous language (Koegel, O’Dell, & Koegel, 1987; Koegel et al., 1989; Laski, Charlop, & Schreibman, 1988; Pierce & Schreibman, 1997; Schreibman & Koegel, 1996). After the student expresses interest in an activity or item, he or she is required to perform a specific behavior related to the item. The consequence of the desired behavior is getting access to the activity or item. For example, students’ attempts to label and request items are reinforced by the delivery of the item, which may then provide the opportunity to focus on other skills, such as joint attention, imitation, play skills, and generalization of other skills learned in the DTT format. FR are the least structured of the STAR instructional strategies. FR strategies are routines that occur throughout the day and include school arrival and dismissal, mealtime, toileting, transitions between classroom activities, and recreational activities. Each routine is broken into discrete steps called a task analysis and then chained together using behavior
- 12. analytic procedures such as stimulus prompts (visual and verbal) and reinforcement of each step in the routine (Brown et al., 1987; Cooper et al., 1987; Marcus et al., 2000; McClannahan & Krantz, 1999). For example, a routine to change activities may include cuing the transition (verbal prompt), checking a schedule (visual prompt), pulling a picture card from the schedule to indicate the next activity, taking the card to the location of Psychology in the Schools DOI: 10.1002/pits Training Teachers in Autism Practices 185 the new activity, putting the card into a pocket utilizing a match-to-sample technique, and beginning the new activity, followed by a token for routine completion. The advantage of this strategy is that each transition component is taught within the context of performing the routine, so that the child learns to respond to natural cues and reinforcers. FR strategies are conducted in both individual and group formats, depending on the skills being taught (e.g., toileting versus appropriate participation in snack time). Training STAR training occurred in accordance with the STAR developers’ training protocols. The research team contracted with the program developers to provide training directly to the teachers. Training included workshops, help with classroom setup, and observation and coaching throughout
- 13. the first academic year of STAR implementation (described in detail in the following sections). Six local coaches also were trained by the STAR developers to provide ongoing consultation to classroom staff during the second year of STAR implementation. The training protocol for STAR is manualized and publicly available. Additional information about the STAR program can be found at www.starautismsupport.com. Training provided to classroom teachers and staff included the following components: Workshops. The STAR program developers provided a series of trainings on the use of the STAR program. The training began in September and consisted of 28 hours of intensive workshops that covered the STAR program, including the use of the curriculum assessment, classroom setup, and training in DTT, PRT, and FR. Workshops included didactic teaching, video examples, role- playing, and a visit to each classroom to help with classroom setup. STAR workshops took place outside the school day (i.e., during professional development days, at night, and on the weekends). Observation and coaching. During the first year, program developers observed classroom staff during regular school hours and provided feedback on use of STAR strategies with students. Trainers provided 5 days of observation and coaching immediately following training, 3 days of follow-up coaching throughout the academic year, and ongoing advising and coaching by e-mail and phone. On average, classrooms received 26.5 (range, 1.5–36) hours of coaching over 5.7 (range, 3–7) visits in the first year. During the second year, local coaches trained
- 14. by the STAR developers provided coaching in the STAR strategies. Coaching was provided September through May on a monthly basis. On average, classrooms received 36.1 (range, 0–59) hours of coaching over 10 (range, 0–10) visits in the second year. Data Collection Procedures Data on adherence to the instructional strategies used in STAR were collected throughout the academic year via video recording of teaching interactions with students for coding of implementa- tion fidelity in each of the three STAR intervention methods. Classroom staff members were filmed for 30 minutes every month in Years 1 and 2. Research assistants trained in filming methods recorded the intervention during a specified date each month. Visits were timed to coincide with regularly scheduled use of each of the intervention methods. The 30-minute film was composed of 10 minutes of DTT, 10 minutes of PRT, and 10 minutes of FR to provide a sample of the use of each intervention. Recording included any consented staff member providing the intervention. The staff member filmed by the research staff varied depending on which staff member (i.e., teacher or paraprofessional) was conducting the intervention that day. The primary classroom teacher conducted the intervention in 86% of the videos collected, and paraprofessional staff conducted the intervention in the remaining 14% of videos. There were no Psychology in the Schools DOI: 10.1002/pits
- 15. 186 Stahmer et al. statistically significant differences in the proportion of videos collected by intervention provider (teacher vs. paraprofessional) for any strategy or time period (p > .05). Implementation Fidelity Measures Coding procedures. The primary method for assessing fidelity of STAR strategies was through video recordings of teachers and aides interacting with students. Coding relied on different criteria based on specific coding definitions created for each instructional component, as well as general teaching strategies (see following sections). Coding schemes for each method were developed by the first author and were reviewed by the STAR program developers. Trained research assistants blinded to the study hypotheses coded all video recordings. For each intervention method, the core research team established correct codes for a subset of videos through consensus coding (keys). Each research assistant coder then learned one coding system (i.e., DTT, PRT, or FR) and was required to achieve 80% reliability across two keys before beginning to code any classroom sessions independently. One third of all tapes were double coded to ensure ongoing reliability of data coding throughout the duration of the project. The core research team also re-coded two tapes for each research assistant every other month, providing a measure of criterion validity. If
- 16. there was less than 80% agreement between the reliability coder and the research assistant, additional training and coaching were provided until criterion was achieved and previous videos were re-coded. Coding involved direct computer entry while viewing videos using “The Observer Video- Pro” software (Noldus Information Technology, Inc., 2008), a computerized system for collection, analysis, and management of direct observation data. For each instructional strategy, the coder observed the 10-minute segment and subsequently rated the adults’ use of each component of the strategy on a 1 to 5 Likert scale, with 1 indicating Adult does not implement throughout segment and 5 indicating Adult implements consistently throughout the segment. These Likert ratings were found to have high concordance with more detailed trial-by-trial coding of each strategy component (88% agreement) used in previous research (Stahmer, 2010). A score of 4 or 5 on a component was considered passing and correlated with 80% correct use of strategies in the more detailed coding scheme. Following are the individual components included in each strategy. Complete coding definitions are available from the first author. Discrete trial teaching. For DTT, coders examined the use of the following components: gaining the student’s attention, choosing appropriate target skills, using clear and appropriate cues, using accurate prompting strategies, providing clear and correct consequences, using appropriate inter-trial intervals, and utilizing error correction procedures effectively (error correction evaluated against procedures described in Arick, Loos, Falco, & Krug,
- 17. 2004). The criterion for passing implementation fidelity was defined as the correct use of 80% of components (score of 4 or 5) during the observation. Pivotal response training. For PRT, coders examined the use of the following components: gaining the student’s attention, providing clear and developmentally appropriate cues related to the activity, providing the student a choice of stimuli/activities, interspersing a mixture of maintenance (previously acquired) and acquisition (not yet mastered) tasks, taking turns to model appropriate be- havior, providing contingent consequences, rewarding goal- directed attempts, and using reinforcers directly related to the teaching activity. The criterion for passing implementation fidelity was defined as the correct use of 80% of components (score of 4 or 5) during the observation. Functional routines. For FR, coders examined adherence to each step of the FR used in class- rooms during group and individual routines. The use of the following components was coded: using error correction procedures appropriately, adhering to FR lesson plan, and supporting transitions Psychology in the Schools DOI: 10.1002/pits Training Teachers in Autism Practices 187 between activities. The criterion for passing implementation fidelity was defined as correct use of 80% of components (score of 4 or 5) during the observation.
- 18. Reliability of Data Recording Inter-rater reliability, as measured by percent agreement within 1 Likert point, was calculated for coding of each instructional strategy and each month of videos by having a second coder, blinded to the initial codes, score one third of the videos per strategy for each month. The average overall percent agreement for each strategy was 86% for DTT (range, 60%–100%); 90% for PRT (range, 75%–100%); and 90% for FR (range, 67%–100%). A primary coder was assigned to each strategy, and those codes were used in the analyses. Data Reduction and Analyses Data were examined across four periods. Time 1 included the first measurement for available classrooms in Year 1, which was conducted in October, November, or December of 2008. Filming occurred after the initial training workshops. Coaching was ongoing throughout the year. If class- rooms were filmed in more than one of those months, both the average and the best performance were analyzed. All classroom staff participated in their initial training prior to the Time 1 measure- ment. Time 2 was defined as the performance from the last three measurements of the school year (February, March, or April 2009) for Year 1. The same procedures were used for Year 2 (Times 3 and 4). Time 3 included the first observation in Year 2 (October, November, or December 2009). Time 4 included the performance during the last 3 months of observations (February, March, or April, 2010). Both average and best performance from each period
- 19. were utilized to provide an estimate of the staff’s capacity to implement the strategy in the classroom environment (best) and variability in competency of use (average). Data from Year 1 and Year 2 were analyzed. One-way within- subject (or repeated measures) analyses of variance (ANOVAs) were conducted for each intervention strategy to examine change in implementation fidelity scores for over time. Post-hoc comparisons were made using paired sample t tests between time periods when ANOVA results indicated statistically significant differences. In addition, we examined differences in fidelity of implementation across intervention strategies using a one-way ANOVA with paired sample t tests to follow up on significant results. Type I error probability was maintained at .05 (two-tailed) for all analyses using a Bonferroni correction. Pearson correlations were conducted to examine the relationship between fidelity of implemen- tation of each intervention strategy and teaching experience, experience working with children with autism spectrum disorder (ASD), level of education, and number of hours of coaching received. RESULTS Use of the Strategies Because teachers who did not allow filming in their classrooms cited staffing difficulties or lack of preparation as the reason, they were considered not to be implementing DTT, PRT, or FR in their classrooms on a regular basis. At Time 1, two teachers
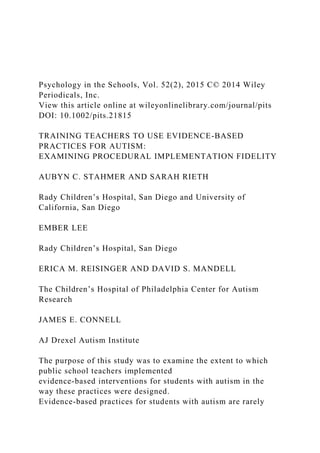
- 20. (4%) explicitly indicated that they did not use DTT at any time, and 13 teachers (23%) indicated that did not use PRT at any time. The percentage of classrooms filmed using the strategy is displayed in Figure 1. In Year 1, classrooms were filmed most often conducting DTT at both Time 1 (70% of classrooms) and Time 2 (96%). Only 23% of classrooms were filmed conducting PRT at Time 1, and 68% were filmed at Time 2. FR was filmed in 67% of classrooms at Time 1 and 81% at Time 2. In Year 2, filming was much more consistent across strategies. DTT and PRT were both filmed in 92% of classrooms at Time 3 Psychology in the Schools DOI: 10.1002/pits 188 Stahmer et al. FIGURE 1. The percentage of classrooms using the strategy during each time period. and 97% of classrooms at Time 4. For FR, 89% of classrooms were filmed at Time 3 and 97% at Time 4. Overall Competence in the Instructional Strategies Discrete trial training. The percentage of DTT components on which teachers met fidelity (i.e., a score of 4 or 5 during the observation) was used as the dependent variable for these analyses. Mean results are displayed in Table 2. No statistically significant changes over time were found in average or best DTT fidelity over time. In general, classrooms
- 21. had a relatively high average and best DTT fidelity during all time periods. The range of scores for individual performance was variable at both time periods, as evidenced by the large standard deviations. The percentage of classrooms in which teachers met DTT fidelity (i.e., correct implementation of 80% of the DTT strategies during the observation) was examined. Fifty-six percent of classrooms met fidelity at Time 1 based on the average of all observations at Time 1, 47% at Time 2, 46% at Time 3, and 59% at Time 4. When considering only the best example, 65% of classrooms met fidelity at Time 1, and this increased to 81% by Time 4 (see Figure 2). Pivotal response training. The dependent variable for these analyses was the percentage of PRT components on which teachers met fidelity (i.e., a score of 4 or 5 during the observation). Mean results are displayed in Table 2. No statistically significant changes were found in average PRT fidelity over time. There was a statistically significant increase in best scores over time, F(3, 108) = 2.85, p = .04. In pairwise comparisons, only the difference in best scores between Time 1 and Time 4 was statistically significant, t(9) = –2.45, p = .04. The range of scores for individual performance was variable at both time periods, as evidenced by the large standard deviations. The percentage of classrooms in which teachers met PRT fidelity was examined (i.e., correct implementation of at least 80% of PRT components during the observation). For average perfor-
- 22. mance, only 15% of classrooms met fidelity at Time 1, 31% at Time 2, 11% at Time 3, and 19% at Time 4. When examining best performance at each time period, 23% of classrooms met fidelity at Time 1, 41% at Time 2, 17% at Time 3, and 30% at Time 4 (see Figure 2). Psychology in the Schools DOI: 10.1002/pits Training Teachers in Autism Practices 189 Table 2 Mean Fidelity of Implementation by Time and Intervention Strategy for Average and Best Fidelitya Intervention Discrete Trial Pivotal Response Functional Overall Teaching Training Routines Fidelity Time M (SD) M (SD) M (SD) M (SD) Average Fidelity across All Assessments During Time Period (%) Time 1 78.54 53.41 56.43 65.14 (24.33) (24.09) (16.42) (16.47) Time 2 73.94 58.43 69.77 68.45 (21.16) (26.66) (19.05) (15.39) Time 3 71.04 68.39 75.56 71.66 (27.79) (20.25) (24.17) (20.01) Time 4 80.46 60.19 78.51 73.58
- 23. (17.55) (21.39) (19.80) (12.98) Best Fidelity for Each Time Period (%) Time 1 81.64 54.64 63.53 69.86 (24.93) (25.60) (20.38) (18.00) Time 2 84.53 65.22 79.96 77.72 (19.77) (23.38) (21.33) (16.28) Time 3 79.21 73.78 81.59 81.33 (26.94) (21.21) (23.78) (11.19) Time 4 90.74 74.16 91.45 85.70 (13.00) (21.96) (16.50) (11.19) aFidelity of implementation is defined as the percentage of strategy components implemented correctly. Teaching in FR. The percentage of FR components on which teachers met fidelity was used as the dependent variable for these analyses. Mean results are displayed in Table 2. Statistically significant changes over time were found in average FR fidelity, F(3, 154) = 9.11, p = .00) and best FR fidelity, F(3, 155) = 12.13, p = .00). The range of scores for individual performance was variable at both time periods, as evidenced by the large standard deviations. Statistically significant increase were seen between Time 1 and each of the other time periods, both for average fidelity (Time 2: t = –3.71, p < .00; Time 3: t = –3.70, p = .00; Time 4: t = –6.14, p = .00), and best fidelity (Time 2: t = –3.83, p < .00; Time 3: t = –3.28, p = .00; Time 4: t = –6.93, p = .00).
- 24. The percentage of classrooms in which teachers met FR fidelity was examined (i.e., correct implementation of 80% FR strategies during the observation). For average performance, 11% of classrooms met fidelity at Time 1, 34% at Time 2, 62% at Time 3, and 49% at Time 4. For best performance, 16% met fidelity at Time 1, and 78% met fidelity by Time 4 (see Figure 2). Overall fidelity. Overall fidelity across the STAR program was examined by averaging the percentage of components implemented correctly in each strategy (DT, PRT, and FR; Table 1). No significant changes over time were seen in the average overall fidelity. However, significant increases in best overall fidelity were indicated, F(3, 178) = 8.14, p = .00). Post-hoc analyses indicated that best fidelity at Time 1 was significantly lower than at any of the other time periods (Time 2: t = –2.72, p < .01; Time 3: t = –4.14, p = .00; Time 4: t = –5.03, p = .00). The range of scores for individual performance was variable at both time periods, as evidenced by the large standard deviations. Psychology in the Schools DOI: 10.1002/pits 190 Stahmer et al. FIGURE 2. Percentage of classrooms meeting 80% implementation fidelity during each time period. FI = fidelity implemen- tation.
- 25. The percentage of classrooms meeting overall fidelity at each time period (i.e., correctly implementing at least 80% of components in all three interventions) was examined. For average performance, 17% of classrooms met fidelity at Time 1, 22% at Time 2, and 42% at both Time 3 and Time 4. For best performance, 31% met fidelity at Time 1, and 71% met fidelity by Time 4 (Figure 2). Comparison of Intervention Fidelity across Intervention Strategies Mean fidelity of implementation was compared across the three intervention strategies for average and best fidelity. Significant differences in average, F(109, 326) = 13.06, p � .00), and best overall fidelity were indicated, F(110, 327) = 3.26, p � .00l (means are presented in Table 2). Analyses indicated that DTT average and best fidelity were significantly greater than were PRT average and best fidelity at Time 2 (average: t = 4.03, p � .00; best: t = 5.14, p � .00) and Time 4 (average: t = –5.46, p � .00; best: t = –4.31, p � .00). FR average and best fidelity were also significantly greater than were PRT average and best fidelity (average: t = 5.46, p � .00; best: t = 4.31, p � .00) at Time 4. Associations between Intervention Fidelity and Experience, Education, or Coaching Pearson correlations indicated there was no statistically significant association between the number of years of either teaching or children with autism and
- 26. overall fidelity or fidelity on any specific intervention strategy at any time point. The number of hours of coaching received was not associated with overall fidelity. Psychology in the Schools DOI: 10.1002/pits Training Teachers in Autism Practices 191 DISCUSSION These results from one of the first field trials of evidence-based practices for students with autism in public schools suggest that classrooms vary greatly in their implementation of evidence- based practices. In general, the data suggest that the complexity and structure of the intervention strategy may affect intervention use and procedural fidelity; more structured methods were more likely to be implemented with higher fidelity than were less structured strategies. Procedural fidelity continued to increase through the second year of training, suggesting the importance of continued practice for extended periods. It is important to note that the number of hours of coaching was not associated with final fidelity, suggesting that in vivo support may be important, but it is not sufficient to improve practice in the field. Classrooms implemented DTT more often in Year 1 and with greater fidelity across both years than PRT or FR. The curriculum materials and steps for implementing DTT are clearly specified, highly structured, and relatively easy to follow. Components
- 27. are, in general, scripted, straightforward, and with the exception of determining appropriate prompting levels, leave little room for clinical judgment. In contrast, PRT is a more naturalistic strategy, and several of the components require clinical judgment on the part of the adult. Teachers had, in general, significantly greater difficulty imple- menting PRT with fidelity than either DTT or FR. During Year 1, many teachers did not implement PRT at all. By Year 2, although they were implementing the strategy, few were doing so with high fidelity. Both average and best fidelity scores across teachers are lower for PRT than either DTT or FR. Teachers may require additional time to develop and integrate these intervention strategies into the school day. It is possible that teachers have difficulty with specific components of PRT that are not well suited to the classroom environment. Recent data indicate that teachers may consistently leave out some components of PRT, which would reduce overall implementation fidelity of the comprehensive model (Suhrheinrich et al., 2013). How these adaptations affect the effectiveness of this intervention is not yet known. FR strategies use many of the procedures of PRT in a group format, but have a specified set of goals and procedures. By the end of Year 2, procedural fidelity was greater for FR than PRT. This may indicate that the structure of the FR, including specific steps and goals, may assist with appropriate implementation of the naturalistic strategies. It may also be helpful that the STAR program uses FR strategies for activities that occur every day (e.g., snack
- 28. time, toileting), providing consistent opportunities to implement the strategy independent of the classroom’s schedule or structure. Relatively high variability across classrooms and over time within classrooms was evident for both use of strategies (as measured by percentage of classrooms filmed) and implementation fidelity. It could be that classroom staff used the strategies with a different child each time they were filmed. Some students may present with behavior challenges that make the use of a particular intervention difficult. Variability in daily staffing, school activities, and student needs may affect the use of intervention strategies on any given day. It is also possible that staff characteristics, such as motivation to implement the intervention, experience, education, and training may affect how well they can use certain methods. Maintenance of all strategies may be difficult, as suggested by the decrease in fidelity at Time 3 (after summer break). Limitations There are several limitations to this study. First, implementation fidelity was examined during brief time periods each month. These data may provide only limited insight into whether strategies were well integrated into the daily classroom routine or used consistently over time or with a majority of students in the classroom. Second, the way fidelity was rated was relatively general and Psychology in the Schools DOI: 10.1002/pits
- 29. 192 Stahmer et al. may not have captured important aspects of the implementation that could affect student progress. Understanding the active ingredients of effective intervention and how to accurately measure those strategies is an area of growth for the field. Third, adults in the classroom knew they were being observed, and this may have altered their use of the strategies. Both the second and third limitations would lead to an overestimate of fidelity. Still, fidelity was relatively low across the three strategies. Strategies may have only been implemented on observation days or may have been implemented differently (better or worse fidelity) during the observations. Fourth, the use of filming as a proxy for use in the classroom has not been validated. In addition, for some observations, paraprofessionals rather than classroom teachers implemented the strategies. A closer examination of differences by profession may be warranted. CONCLUSIONS Results of this study indicate that teachers and staff in public school special education class- rooms can learn to implement structured strategies that are the foundation of many autism interven- tion programs; however, they require a great deal of training, coaching, and time to reach and maintain implementation fidelity. A recent study indicates that ongoing classroom coaching can result in the use of important classroom practices, such as ongoing progress monitoring (Pellecchia et al., 2010). Even with ongoing support, however, not all staff will
- 30. implement interventions with high fidelity. Highly structured strategies appear to be easier to learn, such that practice and coaching may be consistently required for teachers to use more naturalistic strategies with high fidelity. Naturalistic strategies may require additional training or adaptation for classroom environments. Some recent preliminary data indicate that teachers may be better able to implement a classroom-adapted version of PRT (Stahmer, Suhrheunrich, Reed, & Schreibman, 2012). Providers who achieve mastery of intervention strategies are likely to lose those skills or the motivation to use those skills over breaks from teaching; thus, ongoing consultation well past the initial didactic training is likely needed to maintain mastery. The same training and consultation strategy was used for all three practices, but with highly different results. These differential results may be related to the intervention itself or to the fit of the training and consultation model to the specific intervention, teacher, and context. Future Research High-quality implementation of evidence-based practices for children with autism in schools is essential for ensuring the best outcomes for this growing population of children. However, research in this area is just beginning to address the complexity of serving children with ASD using comprehensive and complex methods. The development of low-cost, accurate fidelity of implementation measurement is important for helping to ensure that teachers are accurately using evidence-based interventions. In addition, future research should address the development of training
- 31. methods for naturalistic strategies that address the complexities of using these strategies in classroom settings. Integrating these strategies throughout the school day and for academic tasks can be challenging; yet, they are considered a very effective practice for children with autism. Often, paraprofessional staff spend a great deal of time working with children in the classroom. Specifically examining training needs and fidelity of implementation of paraprofessional staff compared with teachers and other professionals is needed. In addition, there are multiple interventions for ASD that are “branded” by various research groups. Often, the specific techniques or strategies overlap significantly. Research examining the key ingredients necessary for effective classroom intervention is sorely needed. This has the potential to simplify and clarify intervention for use by teachers and other community providers. Psychology in the Schools DOI: 10.1002/pits Training Teachers in Autism Practices 193 REFERENCES Arick, J. R., Loos, L., Falco, R., & Krug, D. A. (2004). The STAR program: Strategies for teaching based on autism research. Austin, TX: Pro-Ed. Brown, F., Evans, I., Weed, K., & Owen, V. (1987). Delineating functional competencies: A component model. Journal of the Association for Persons with Severe Handicaps, 12, 117–
- 32. 124. Bush, R. N. (1984). Effective staff development. San Francisco, CA: Far West Laboratory for Educational Research and Development. Cooper, J. O., Heron, T. E., & Heward, W. L. (1987). Applied behavioral analysis. New York, NY: Macmillan. Cornett, J., & Knight, J. (2009). Research on coaching. In J. Knight (Ed.), Coaching: Approaches and perspectives (pp. 192–216). Thousand Oaks, CA: Corwin Press. Dingfelder, H. E., Mandell, D. S., & Marcus, S. C. (2011, May). Classroom climate program fidelity & outcomes for students with autism. Paper presented at the 10th annual International Meeting for Autism Research. San Diego, CA. Durlak, J. A., & DuPre, E. P. (2008). Implementation matters: A review of research on the influence of implementation on program outcomes and the factors affecting implementation. American Journal of Community Psychology, 41, 327–350. Fenske, E., Krantz, P. J., & McClannahan, L. E. (2001). Incidental teaching: A non-discrete trial teaching procedure. In C. Maurice, G. Green, & R. Foxx (Eds.), Making a difference: Behavioral intervention for autism (pp. 75–82). Austin, TX: Pro-Ed. Garland, A. F., Bickman, L., & Chorpita, B. F. (2010). Change what? Identifying quality improvements targets by investigating usual mental health care. Administration and Policy in Mental Health and Mental Health Services Research, 37, 15–26. Gersten, R., Fuchs, L., Compton, D., Coyne, M., Greenwood,
- 33. C., & Innocenti, M. S. (2005). Quality indicators for group experimental and quasi-experimental research in special education. Exceptional Children, 71, 149–164. Gresham, F. M. (1989). Assessment of treatment integrity in school consultation and prereferral intervention. School Psy- chology Review, 18, 37–50. Gresham, F. M. (2009). Evolution of the treatment integrity concept: Current status and future directions. School Psychology Review, 38, 533–540. Gresham, F. M., Gansle, K. A., & Noell, G. H. (1993). Treatment integrity in applied behavior analysis with children. Journal of Applied Behavior Analysis, 26, 257–263. Gresham, F. M., MacMillan, D. L., Beebe-Grankenberger, M. E., & Bocian, K. M. (2000). Treatment integrity in learning disabilities intervention research: Do we really know how treatments are implemented? Learning Disabilities Research and Practice, 15, 198–125. Harn, B., Parisi, D., & Stoolmiller, M. (2013). Balancing fidelity with flexibility and fit: What do we really know about fidelity of implementation in schools? Exceptional Children, 79, 181–193. Hess, K. L., Morrier, M. J., Heflin, L. J., & Ivey, M. L. (2008). Autism treatment survey: Services received by children with autism spectrum disorders in public school classrooms. Journal of Autism and Developmental Disorders, 38, 961–971. Horner, R. H., Carr, E. G., Halle, J., McGee, G. G., Odom, S. L., & Wolery, M. (2005). The use of single-subject research to
- 34. identify evidence-based practice in special education. Exceptional Children, 71, 165–179. Jennett, H. K., Harris, S. L., & Mesibov, G. B. (2003). Commitment to philosophy, teacher efficacy, and burnout among teachers of children with autism. Journal of Autism and Developmental Disorders, 33, 583–593. Koegel, R. L., O’Dell, M. C., & Koegel, L. K. (1987). A natural language teaching paradigm for nonverbal autistic children. Journal of Autism & Developmental Disorders, 17, 187–200. Koegel, R. L., Russo, D. C., & Rincover, A. (1977). Assessing and training teachers in the generalized use of behavior modification with autistic children. Journal of Applied Behavior Analysis, 10, 197–205. Koegel, R. L., Schreibman, L., Good, A., Cerniglia, L., Murphy, C., & Koegel, L. K. (Eds.). (1989). How to teach pivotal behaviors to children with autism: A training manual. Santa Barbara: University of California–San Diego. Krug, D. A., Arick, J., Almond, P., Rosenblum, J., Scanlon, C., & Border, M. (1979). Evaluation of a program of systematic instructional procedures for pre-verbal autistic children. Improving Human Performance, 8, 29–41. Krug, D. A., Rosenblum, J. F., Almond, P. J., & Arick, J. R. (1981). Autistic and severely handicapped in the classroom: Assessment, behavior management, and communication training. Portland, OR: ASIEP Education. Laski, K. E., Charlop, M. H., & Schreibman, L. (1988). Training parents to use the natural language paradigm to increase
- 35. their autistic children’s speech. Journal of Applied Behavior Analysis, 21, 391–400. Leaf, R. B., & McEachin, J. J. (1999). A work in progress: Behavior management strategies and a curriculum for intensive behavioral treatment of autism. New York, NY: DRL Books. Lovaas, O. I. (1981). Teaching developmentally disabled children: Theme book. Austin, TX: PRO-ED. Lovaas, O. I. (1987). Behavioral treatment and normal educational and intellectual functioning of young autistic children. Journal of Consulting and Clinical Psychology, 55, 3–9. Lovaas, O. I. (2003). Teaching individuals with developmental delays: Basic intervention techniques. Austin, TX: Pro-Ed. Psychology in the Schools DOI: 10.1002/pits 194 Stahmer et al. Lovaas, O. I., & Buch, G. (1997). Intensive behavioral intervention with young children with autism. In N. Singh (Ed.), Prevention and treatment of severe behavior problems: Models and methods in developmental disabilities (pp. 61–86). Pacific Grove, CA: Brooks/Cole Publishing. Mandell, D. S., Stahmer, A. C., Shin, S., Xie, M., Reisinger, E., & Marcus, S. C. (2013). The role of treatment fidelity on outcomes during a randomized field trial of an autism intervention. Autism, 17, 281–295. Marcus, L., Schopler, E., & Lord, C. (2000). TEACCH services for preschool children. In J. S. Handleman & S. L. Harris
- 36. (Eds.), Preschool education programs for children with autism (pp. 215–232). Austin, TX: Pro-ED. McClannahan, L. E., & Krantz, P. J. (1999). Activity schedules for children with autism: Teaching independent behavior. Bethesda, MD: Woodbine House. McIntyre, L. L., Gresham, F. M., DiGennaro, F. D., & Reed, D. D. (2007). Treatment integrity of school-based interventions with children in the Journal of Applied Behavior Analysis 1991–2005. Journal of Applied Behavioral Analysis, 40, 659–972. National Standards Project. (2009). National Standards report. Randolph, MA: National Autism Center. Noell, G. H., Duhon, G. J., Gatti, S. L., & Connell, J. E. (2002). Consultation, follow-up and implementation of behavior management interventions in general education. School Psychology Review, 31, 217–234. Noell, G. H., Witt, J. C., Slider, N. J., Connel, J. E., Williams, K. L., Resetar, J. L., & Koenig, J. L. (2005). Teacher implementation following consultation in child behavior therapy: A comparison of three follow-up strategies. School Psychology Review, 37, 87–106. Noldus Information Technology, Inc. (2008). The Observer XT 8.0 [computer software]. Wageningen, The Netherlands. Odom, S. L., Boyd, B. A., Hall, L. J., & Hume, K. (2010). Evaluation of comprehensive treatment models for individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 40, 425–436. Odom, S. L., & Wolery, M. (2003). A unified theory of practice in early intervention/early childhood special education:
- 37. Evidence-based practices. Journal of Special Education, 37, 164–173. Pellecchia, M., Connell, J. E., Eisenhart, D., Kane, M., Schoener, C., Turkel, K., & Mandell, D. S. (2010). Group performance feedback: Consultation to increase classroom team data collection. Journal of School Psychology, 49, 411–431. Peterson, L., Homer, A. L., & Wonderlich, S. A. (1982). The integrity of independent variables in behavior analysis. Journal of Applied Behavior Analysis, 15, 477–492. Pierce, K., & Schreibman, L. (1997). Multiple peer use of pivotal response training to increase social behaviors of classmates with autism: Results from trained and untrained peers. Journal of Applied Behavior Analysis, 30, 157–160. Proctor, E., Simere, H., Raghavan, R., Hovmand, P., Aarons, G., Bunger, A., & Hensley, M. (2011). Outcomes for imple- mentation research: Conceptual distinctions, measurement challenges, and research agenda. Administration and Policy in Mental Health and Mental Health Services Research, 38, 65– 76. Rabin, B. A., Brownson, R. C., Haire-Joshu, D., Kreuter, M. W., & Weaver, N. L. (2008). A glossary for dissemination and implementation research in health. Journal of Public Health Management and Practice, 14, 117–123. Sarokoff, R. A., & Sturmey, P. (2004). The effects of behavioral skills training on staff implementation of discrete-trial teaching. Journal of Applied Behavior Analysis, 37, 535–538.
- 38. Schoenwald, S. K., Garland, A. F., Chapman, J. E., Frazier, S. L., Sheidow, A. J., & Southam-Gerow, M. A. (2011). Toward the effective and efficient measurement of implementation fidelity. Administration and Policy in Mental Health and Mental Health Services Research, 38, 32–43. Schreibman, L., & Koegel, R. L. (1996). Fostering self- management: Parent-delivered pivotal response training for children with autistic disorder. In E. D. Hibbs & P. S. Jensen (Eds.), Psychosocial treatments for child and adolescent disorders: Empirically based strategies for clinical practice (pp. 525–552). Washington, DC: American Psychological Association. Scull, J., & Winkler, A. M. (2011). Shifting trends in special education. Washington, DC: Thomas B. Fordham Institute. Simpson, R. L., de Boer-Ott, S. R., & Smith-Myles, B. (2003). Inclusion of learners with autism spectrum disorders in general education settings. Topics in Language Disorders, 23, 116–133. Sindelar, P. T., Brownell, M. T., & Billingsley, B. (2010). Special education teacher education research: Current status and future directions. The Journal of the Teacher Education Division of the Council for Exceptional Children, 33, 8–24. Smith, T. (2001). Discrete trial training in the treatment of autism. Focus on Autism and Other Developmental Disabilities, 16, 86–92. Smith, T., Buch, G. A., & Gamby, T. E. (2000). Parent-directed, intensive early intervention for children with pervasive developmental disorder. Research in Developmental Disabilities, 21, 297–309. Smith, T., Donahoe, P. A., & Davis, B. J. (2000). The UCLA young autism project. Austin, TX: Pro-Ed.
- 39. Smith, T., Parker, T., Taubman, M., & Lovaas, O. I. (1992). Transfer of staff training from workshops to group homes: A failure to generalize across settings. Research in Developmental Disabilities, 13, 57–71. Stahmer, A. (2007). The basic structure of community early intervention programs for children with autism: Provider descriptions. Journal of Autism and Developmental Disorders, 37, 1344–1354. Stahmer, A. (2010). Examining methods of fidelity of implementation measurement. Unpublished raw data. Psychology in the Schools DOI: 10.1002/pits Training Teachers in Autism Practices 195 Stahmer, A., Collings, N. M., & Palinkas, L. A. (2005). Early intervention practices for children with autism: Descriptions from community providers. Focus on Autism & Other Developmental Disabilities, 20, 66–79. Stahmer, A., & Gist, K. (2001). The effects of an accelerated parent education program on technique mastery and child outcome. Journal of Positive Behavior Interventions, 3, 75–82. Stahmer, A., & Ingersoll, B. (2004). Inclusive programming for toddlers with autism spectrum disorders: Outcomes from the Children’s Toddler School. Journal of Positive Behavior Interventions, 6, 67–82. Stahmer, A., Suhrheinrich, J., Reed, S., Bolduc, C., & Schreibman, L. (2011). Classroom pivotal response teaching: A guide
- 40. to effective implementation. New York, NY: Guilford Press. Stahmer, A. C., Suhrheinrich, J., Reed, S., & Schreibman, L. (2012). What works for you? Using teacher feedback to inform adaptations of pivotal response training for classroom use. Autism Research and Treatment, 2012, 1–11. Suhrheinrich, J. (2011). Training teachers to use pivotal response training with children with autism; Coaching as a critical component. Teacher Education and Special Education, 34, 339– 349. Suhrheinrich, J., Stahmer, A., Reed, S., Schreibman, L., Reisinger, E., & Mandell., D. (2013). Implementation challenges in translating pivotal response training into community settings. Journal of Autism and Developmental Disorders, 43, 2970–2976. Swanson, E., Wanzek, J., Haring, C., Ciullo, S., & McCulley, L. (2011). Intervention fidelity in special and general education research journals. The Journal of Special Education, 47, 13–33. Wheeler, J. J., Baggett, B. A., Fox, J., & Blevins, L. (2006). Treatment integrity: A review of intervention studies conducted with children with autism. Focus on Autism and Other Developmental Disabilities, 21, 1–10. Wolery, M., & Garfinkle, A. N. (2002). Measures in intervention research with young children who have autism. Journal of Autism and Developmental Disorders, 32, 463–478. Psychology in the Schools DOI: 10.1002/pits
- 41. Copyright of Psychology in the Schools is the property of John Wiley & Sons, Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. Medical Case Study with Minitab for solutions Background: You work for a government agency and your management asked you to take a look at data from prescription drugs administered at hospitals in your geography. She asked you to analyze the data with some common tools and build a DMAIC model for how you would work with the hospitals to improve results, since their performance is below the average. She would like a simple model for you to present to her that you will propose to representatives from the hospitals. The hospital representatives will have to be brought on board and understand the issues and their role in the study. Use the DMAIC model from the course material to create a model of the effort to be completed by the hospitals. Define: 1. What would you say about the DMAIC model to the hospital staff on your team? 2. Write a problem statement for the work you are considering. 3. Develop a team charter so that each of the representatives understands what is expected of them and to brainstorm improvements upon it. 4. What are the key deliverables of the define step that you expect of the team?
- 42. Measure: 1. What activities would you propose that the team work on? 2. What measures would you propose to the team to pursue? 3. What data collection would you propose? 4. What are the key steps to get to items 1-3 above? Analyze: Prepare data to show the team about the extent of the problem: 1. A Pareto chart of the errors from the Error Type chart below 1. What would you suggest the team focus upon? 2. What would you tell the team about the data they need to collect and what will be done with it? 2. Another example of measures is the administration of Drug A, which needs to be administered every 30 minutes. The requirement for the drug is to be administered no more than 3 minutes early or 3 minutes late or between 27-33 minutes. Make a histogram of the data below (Time between administration of drug chart). What is it saying about the process? 3. Do a normalcy test. Is that a normal distribution?
- 43. Improve: 1. You don’t have a process flow or any information on how hospitals administer drugs or their improvement plans if any. What would you tell the participants about what is expected in this phase of the program?
- 44. Control: 1. What are the key steps for control? 2. Develop a sample response plan that you would use to show the team what is expected to be done. 3. What are the key deliverables for this step? Test data in Excel format: Error Type Type of High Alert Medication Error Omission 8461 Improper dose/quantity 7124 Unauthorized/wrong drug 5463 Prescribing error 2923 Wrong Time 2300 Extra Dose 2256 Wrong patient 1786 Mislabeling 636 Wrong dosage form 586 Wrong administration 335 Drug prepared incorrectly 311 Wrong route 252 Other
- 45. 113 32546 Observation Time between administration of Drug 1 35.5 2 26.2 3 31.6 4 26.4 5 28.5 6 24.6 7 26.1 8 29.4 9 33.6 10 38.8 11 27.0 12
- 48. 25.0 49 24.6 50 40.0 1 The Journal of Special Education 2016, Vol. 50(1) 27 –36 © Hammill Institute on Disabilities 2015 Reprints and permissions: sagepub.com/journalsPermissions.nav DOI: 10.1177/0022466915613592 journalofspecialeducation.sagepub.com Article In the field of special education, a commitment to the logic and ethics of using research to inform decisions about prac- tice has been reflected in the field’s efforts to identify and use evidence-based practices (EBPs) as a standard for the profession (Council for Exceptional Children, 2014; Odom et al., 2005). As in other fields, this focus has led inexorably back to what some commentators have termed the “wicked” problem of implementation (Cook & Odom, 2013). Fixen and his colleagues (following Rittel & Webber, 1973) described wicked problems as those that are “difficult to define and fight back when you try to solve them” (Fixen, Blaze, Metz, & Van Dyke, 2013, p. 218). Indeed, the obser-
- 49. vation that “interests vested in the system-as-is suddenly appear and typically deter attempts to change the system” (Fixen et al., 2013, p. 218) has been made by ecologically oriented observers of human behavior since time of Marx (Bronfenbrenner, 1979; Lewin, 1951; Marx, 1888/1984). One implication of this view, of course, is that the problem of (non)implementation of EBP may be most usefully viewed not simply as a “deficit” in the knowledge, skills, or ideological commitments of practitioners but as a product of the set of social, organizational, and material conditions that operate in a given human service setting. In this article, we draw on interviews conducted with special education practitioners to investigate how these kinds of contextual factors (and others) may affect the ways in which practitio- ners interpret and respond to contemporary press for imple- mentation of EBP. We are by no means the first to recognize the importance of seeking practitioner perspectives in understanding the challenges of implementing EBP in special education. For example, Landrum, Cook, Tankersley, and Fitzgerald (2002) surveyed 127 teachers (60 special educators, 67 general edu- cators) to assess their views about the value of four sources of information about practice: university coursework, 613592 SEDXXX10.1177/0022466915613592The Journal of Special EducationHudson et al. research-article2015 1University of Washington, Seattle, USA 2Northern Illinois University, DeKalb, USA 3Central Michigan University, Mount Pleasant, USA 4American Institutes for Research, Washington, DC, USA Corresponding Author:
- 50. Roxanne F. Hudson, Area of Special Education, University of Washington, P.O. Box 353600, Seattle, WA 99195, USA. E-mail: [email protected] A Socio-Cultural Analysis of Practitioner Perspectives on Implementation of Evidence-Based Practice in Special Education Roxanne F. Hudson, PhD1, Carol A. Davis, EdD1, Grace Blum, MEd1, Rosanne Greenway, MEd1, Jacob Hackett, MEd1, James Kidwell, MEd1, Lisa Liberty, PhD1,2, Megan McCollow, PhD1,3, Yelena Patish, MEd1, Jennifer Pierce, PhD1,4, Maggie Schulze, MEd1, Maya M. Smith, PhD1, and Charles A. Peck, PhD1 Abstract Despite the central role “evidence-based practice” (EBP) plays in special education agendas for both research and policy, it is widely recognized that achieving implementation of EBPs remains an elusive goal. In an effort to better understand this problem, we interviewed special education practitioners in four school districts, inquiring about the role evidence and EBP played in their work. Our data suggest that practitioners’ responses to policies that press for increased use of EBP are mediated by a variety of factors, including their interpretations of the EBP construct itself, as well as the organizational conditions of their work, and their access to relevant knowledge and related tools to support implementation. We interpret these findings in terms of their implications for understanding the problem of implementation through a more contextual and ecological lens than has been reflected in much of the literature to date.
- 51. Keywords evidence-based practices, implementation, special education practitioners mailto:[email protected] http://crossmark.crossref.org/dialog/?doi=10.1177%2F00224669 15613592&domain=pdf&date_stamp=2015-11-08 28 The Journal of Special Education 50(1) research journals, teaching colleagues, and in-service/pro- fessional development workshops. Their data indicated that research journals and university courses (presumably sources of relatively reliable information about EBP) were viewed as less useful, less trustworthy, and less accessible than either information from colleagues or information received via professional development. Similarly, Boardman, Argüelles, Vaughn, Hughes, and Klingner (2005) reported that teachers often expressed the belief that the extant research was not relevant to the populations they served in their classrooms, and reported relying on colleagues for rec- ommendations about practice. In a more recent study, Jones (2009) investigated the views of 10 novice special educators regarding EBP. Based on interview, classroom observation, and rating scale data, Jones suggested that the novice teachers she studied fell into three broad groups. “Definitive supporters” expressed clear and positive views about the importance of research in decisions about classroom practice. “Cautious consumers” felt research could be useful, but often did not reflect char- acteristics and needs of their individual students. A third group, “The Critics,” expressed skepticism about the value of research for decisions about classroom practice.
- 52. Taken together, these studies (and others) provide a rather robust picture of the tensions between research and practice in special education. While significant variation exists among special education practitioners in their views about the value and relevance of research to their work in the classroom, many express more confidence in the knowl- edge and expertise of local colleagues than in information they might receive from university coursework and/or researchers. This result is consistent with research from other fields and suggests that much remains to be learned about the conditions under which practitioners utilize knowledge from research in decisions about practice (Aarons & Palinkas, 2007; Glasgow, Lichtenstein, & Marcus, 2003). In our review of the special education research on this topic, we noted that most researchers have framed their analysis of practitioner perspectives related to implementa- tion of EBP in essentially individualistic and personological terms—placing teachers (and, in some cases, administra- tors) in the center of their analysis of the implementation process. For example, as noted earlier, Jones (2009) parsed individual teachers into groups such as “the Critics” and “the Supporters.” Also focusing on individual practitioners, Landrum et al. (2002) argued, Only when we have confidence that teachers learn about empirically sound practice in both their initial preparation and ongoing professional development, and that their skills reflect this training, can we predict that students with disabilities will be afforded the most appropriate learning opportunities available. (p. 48) We do not entirely disagree with these conclusions, and others like them that underscore the importance of persono- logical variables (e.g., practitioner knowledge, prior train-
- 53. ing, attitudes) affecting implementation of EBP. But we would also argue that in foregrounding characteristics of individual practitioners as a focus of analysis, these studies reflect a set of implicit assumptions about the nature of practice and how it is constructed that narrows our view of the problems of implementation, and the range of actions to be considered in engaging those problems. In the present study, we follow recent recommendations (Harn, Parisi, & Stoolmiller, 2013; Klingner, Boardman, & McMaster, 2013; Peck & McDonald, 2014) in undertaking a more holistic and contextual approach to understanding how practitioner perspectives on EBP are shaped by the conditions in which they work. Theoretical Framing In conceptualizing “a more contextual” approach to under- standing practitioner interpretation and implementation of EBP, we drew on some of the precepts of sociocultural the- ory as a general framework for investigating ways in which social and material conditions shape workplace learning and practice (Billett, 2003; Engeström, 2001; Scribner, 1997; Vygotsky, 1978). Our choice of a sociocultural per- spective was based on several of its key precepts that we believed would be useful in understanding practitioner per- spectives on implementation of EBP. First, sociocultural theory foregrounds analysis of relationships between indi- vidual and collective dimensions of social practice—in this case, the analysis of the transactions that take place between individual practitioners and the organizations in which they work (Engeström, 2001). Second, this view assumes that human thought processes (including, of course, one’s views about EBP) are shaped by the demands of the practical activities in which people are regularly engaged. A third assumption of this stream of sociocultural theory is that par- ticipation in social practice is affected by the affordances
- 54. and constraints of the conceptual and material tools avail- able (e.g., the characteristics and representations of EBP available in local school districts and other professional resources; Falmagne, 1995; Leontev, 1975/1978; Scribner, 1997). Overall, the sociocultural perspective suggests the value of undertaking a more focused analysis of the social and organizational conditions in which decisions about practice are made than has been reflected in much of the extant research on the problem of implementation. We used the following research questions to guide our inquiry: Research Question 1: How do special education practi- tioners interpret the meaning of EBP in the context of decisions they make about curriculum and instruction? Hudson et al. 29 Research Question 2: What contextual factors are asso- ciated with practitioner interpretations of the role EBP can and should play in their decisions about instruction? Method We used a qualitative methodology (Merriam, 2009) to investigate the perspectives—that is, the values, beliefs, and attitudes—held by special education practitioners with regard to their views about EBP, and the role research played in their decisions about curriculum and instruction. We elected this methodological approach because of the hypothesis-generating, rather than hypothesis-testing, pur- poses of the study (Glaser & Strauss, 1967). Participants
- 55. A total of 27 special education practitioners participated in our study. We contacted directors of special education via email and invited participation from four school districts in the Seattle/Puget Sound area. Demographics for these dis- tricts are presented in Table 1. Teacher participants were nominated by special educa- tion directors, who were asked to identify individuals they believed would be interested in being interviewed for the study. In each district, we requested nominations of teachers working in three types of programs or settings: resource rooms serving students with a wide range of disability labels placed primarily in general education classrooms, self-contained classes serving students with emotional/ behavioral disabilities (EBD), and self-contained class- rooms serving students with low-incidence developmental disabilities. Table 2 reports the number, working context, and experience level of study participants in each of the dis- tricts in which we collected data. Data Collection and Analysis Interviews. The primary data source for our study consisted of face-to-face interviews we conducted individually with the 27 special educators who agreed to participate in the study. We used semistructured interview protocols for each of the four types of practitioners we interviewed: special education directors, resource room teachers, EBD teachers, and teachers of students with low-incidence developmental disabilities. While the protocols for administrators and teachers varied in some ways, both were structured to pro- ceed from general, context-descriptive questions such as “Tell me about the work you do,” to more focused questions about daily practice (“Tell me about a typical day in your classroom”). We asked each informant to define the term
- 56. EBP and tell us what it meant to them in terms of their deci- sions about curriculum and instruction. Interview protocols also included a series of questions about district policies related to EBP in both general and special education, and how these affected the decisions our informants made in the classroom. Interviews were generally between 45 min to an hour in length. Interviews were audio-recorded and subse- quently transcribed verbatim for analysis. Transcripts were entered into a web-based platform for qualitative and mixed-method data analysis (http://www.dedoose.com). Data analysis. We used the standard procedures for induc- tive data analysis described by Charmaz (2002), Strauss and Corbin (1997), and others. Thus, we began our analysis by having each of the 11 members of our research team read through the interview transcripts, identifying text segments of potential relevance to our research questions. Each of these segments was tagged using low inference descriptors, such as “classroom assessment” or “progress monitoring.” Members of the research team then met to discuss examples of the text segments they had tagged, identifying and defin- ing codes emerging from individual analysis to be formal- ized and used collectively. The remainder of the interviews were then coded, followed by an additional round of team meetings in which examples of each code were discussed, with some codes combined, others modified or deleted based on their perceived value relative to our research ques- tions. A set of interpretive categories were developed through this process which were used to aggregate coded data segments and which became the basis for further anal- ysis. These categories were then used as a basis for develop- ing a series of data displays (Miles & Huberman, 1994) organized by district and by each type of participant (i.e., resource room teachers, special education directors, etc.). Team members met to discuss the implications of these analyses and to develop a set of analytic memos which inte-
- 57. grated the categorical data into larger and more interpretive case summaries. These summaries were used to develop the set of cross-case findings described below. Results Our findings suggest that personal characteristics (particu- larly values and beliefs about EBP), the features of organi- zations (particularly practitioner positionality within these organizations), and access to relevant tools all affected the Table 1. School District Characteristics. District Enrollment Special education enrollment (%) Students eligible for free or reduced-price meals (%) A 18,123 9.70 22.10 B 20,659 13.60 35.10 C 17,973 13.60 66.90 D 8,920 12.40 26.00 http://www.dedoose.com 30 The Journal of Special Education 50(1) ways practitioners interpreted the relevance of the EBP to decisions they made about practice. We interpreted these as dimensions of practical activity that were inseparable and mutually constitutive (Billett, 2006). As depicted in
- 58. Figure 1, our data suggest these factors operate in a highly interdependent manner. We use this conceptual model to understand both the points of the triangle and the interac- tions that take place between points as represented by the lines of the triangle. In the following sections, we will present findings both related to the points of the triangle and the intersections of elements. First, we use excerpts from our interviews to illustrate how the practitioners we interviewed interpreted the idea of EBP, the organizational contexts they worked in, and the tools and resources available to them. Second, we present findings that illuminate the connections and interac- tions between them. People: Practitioner Definitions of EBP We asked each of our informants how they defined EBP in the context of their work in special education. The predomi- nance of responses to this question reflected the notion that EBP meant that “someone” had researched a specific pro- gram or practice and found it to be effective: There’s obviously been research and studies so what I picture in my mind is that they have a curriculum and they conduct a study where they have kids who participate in the study and then they probably have some pre- and posttest to see if they’ve made gains. I’d say evidence-based would be like, that it’s been tried in lots of different settings, across you know lots of different populations and there’s been demonstrated success using that curriculum or whatever the thing is you’re talking about, you know, the social skills sheet or something. So it’s used with lots of people and over different settings.
- 59. We noticed that our participants typically defined EBP in ways that emphasized its external origins, and its ostensive function as a “prescription” for their practice, rather than as a resource for their own decision making (Cook & Odom, 2013). In some cases, this interpretation was also congruent with the stance taken by district administrators: We have adults that want to continue to do what they’ve done in the past. And it is not research-based nor if you look from a data perspective has it been particularly effective and that’s not going to happen and we say, “This is the research, this is what you’re going to do.” (Special Education Director, District A) This strong ideological commitment to use of EBP in the classroom was shared by some teachers: I believe that by using research-based instruction, and teaching with fidelity, then you’re more likely to have an outcome that is specific to the research, as long as we use the curriculum as it’s designed. Um, I think it’s vital, I think it’s vital that we are not pulling things out of a hat, that we are using. (Resource Room Teacher, District A) More often, however, we found that practitioner views about research in general, and the value of EBP in decision making about classroom practice in particular, were more ambivalent. Perhaps the most widely shared concern about EBP expressed by our informants had to do with the ten- sions they perceived between the “general case” and the specifics of local context, including the special needs of the children served in the schools and classrooms in which they worked (Cook, Tankersley, Cook, & Landrum, 2008). While the value of research and the relevance of EBP were often acknowledged in abstract terms, both teachers and administrators were quick to identify what they perceived
- 60. to be limitations in the relevance of research for local deci- sion making and special populations: . . .well what makes me question it—I’m always curious about what the norm population is because it is talking about typically developing kids and research-based practices that are used for those types of kids. It’s very different for my kids. So when I’m looking at an evidenced-based practice I want to be clear on what evidence [is about] Gen Ed versus the Special Ed population. (Self-Contained Classroom Teacher, District B) Table 2. Participant Characteristics. Participants Number of participants per district Median years in position District Special education director EBD teacher Resource room teacher Self-contained teacher A 1 1 2 2 6 7 B 1 1 2 3 7 10
- 61. C 1 2 2 2 7 6 D 1 2 2 2 7 6 Note. EBD = emotional/behavioral disabilities. Hudson et al. 31 For many teachers, ambivalence about EBP included particular tension about who makes decisions about the rel- evance of evidence to their classroom practice. These teach- ers often made reference to local perspectives as “forgotten” or “overlooked” in decisions about practice: . . . evidence-based is very important because you do need to look at what you’re doing but there is just the day-to-day knowledge that is overlooked in the evidence-based piece. (Self-Contained Classroom Teacher, District B) Most of the teachers and many administrators we inter- viewed appeared to locate the authority for making evi- dence-based decisions about curriculum and instruction with the district central office or with “general education.” For example, one director of special education reported, “for our resource room students . . . we always start with the Gen Ed and then if we have curriculum, if a part of that cur- riculum has a supported intervention component to it we start with that.” Many teachers similarly viewed the locus of decisions about curriculum and instruction as external to their classrooms. As a Resource Room Teacher in District D puts it, They tell us what to teach and when to teach it. I mean, we have a calendar and a pacing guide. We can’t, we really don’t make the decisions too much. I would hope . . . that it’s
- 62. supported and making sure that students learn but I don’t really know. In some cases, these teachers expressed confidence that the judgments of district curriculum decision makers were grounded in appropriate evidence: I kind of just trust that the district is providing me with evidence-based stuff. So I’m trusting that the curriculum that they’ve chosen and that my colleagues have done test work on is really what they say it is. (EBD Teacher, District D) However, in other cases, teachers expressed more skepti- cal views about the trustworthiness of the data district offi- cials used to make decisions about curriculum: . . . over the years we’ve had so many evidence-based, research based and so many changes, that . . . if you just want my honest [opinion] . . . I know that there’s data behind it, but if it’s evidence based or research based, why are we always changing? (EBD Teacher, District B) Figure 1. Relationships between people, organizations, and tools. Adapted from McDiarmid & Peck (2012). 32 The Journal of Special Education 50(1) To summarize, similar to earlier studies (Boardman et al., 2005; Jones, 2009; Landrum et al., 2002), we found that the personal characteristics of practitioners—that is, their experiences, values, beliefs, and attitudes—functioned as a powerful filter through which they interpreted the meaning of EBP and evaluated the relevance of this con- struct for their decision making about curriculum and
- 63. instruction. Practitioner definitions of EBP often reflected the assumption that the locus of authority regarding EBP lies outside the classroom, and the ostensive function of EBP was to provide prescriptions for classroom practice. In the following sections, we report findings related to our second research question, describing ways in which contextual features such as organization and access to tools and resources may influence the way practitioners interpret the value and relevance of EBP in their daily work. Organizational Contexts of EBP Our data suggest that our interviewees’ views about the value and relevance of evidence in decision making about practice were often part of a larger process of coping with the organizational conditions of their work. Several specific issues were salient in the interviews we conducted. One of these, of course, had to do with district policies about evi- dence-based decision making (Honig, 2006). In some dis- tricts, special education administrators described strong district commitments related to the use of research evidence in decision making: In this district, it’s [EBP] becoming really big. You don’t ever hear them talk about any initiative without looking at the research and forming some sort of committee to look at what practices are out there and what does the research tell us about it. And then identifying what are the things we’re after and how well does this research say they support those specific things we want to see happen. I would say that work has started, and that is the lens that comes from Day One of anything we do. (Special Education Administrator, District C) However, strong district commitments to evidence-based curriculum decisions in general education were sometimes
- 64. viewed as raising dilemmas for special education teachers. A teacher of students with emotional and behavioral prob- lems in District B described the problem this way: I try to make our classroom setting as much like a general Ed classroom as I can, because the goal is to give them strategies to work with behaviors so that they can function in Gen Ed classrooms. Which is a challenge, because they were in Gen Ed classrooms before they came here, so something wasn’t working. Some special education teachers described being caught between curriculum decisions made in general education and practices they saw as more beneficial for their students with disabilities: . . . if (general education teachers) change their curriculum then I need to follow it so my kids can be a part of it. Especially with my kids being more part of the classroom. So you know 4 years ago I was not doing the Math Expressions, and now I am doing the Math Expressions and it’s hard because I’m trying to follow the Gen Ed curriculum and there’s times where the one lesson ends up being a 2- or 3-day lesson with some added worksheets because they just aren’t getting the skill and, being a spiraling curriculum, it goes pretty fast sometimes too. (Self-Contained Teacher, District B) While the tensions between curriculum models in gen- eral education and special education (with each claiming its own evidentiary warrants) were problematic for many of the resource room teachers we interviewed, these dilemmas were less salient to teachers of children in self-contained classrooms, including those serving students with EBD and those serving students with low-incidence disabilities. Instead, the challenges that these teachers described had to
- 65. do with isolation and disconnection from colleagues serv- ing students like theirs. A Self-Contained Classroom Teacher, District B, said, “Well, this job is very isolating. I’m the only one that does it in this building . . . so uh I’m kind of alone in the decisions I make.” Another Self- Contained Classroom Teacher, District D, said, Sometimes it makes me feel like it’s less than professional . . . I don’t know, I just sometimes wish that, I feel like there’s not always a lot of oversight as far as what am I doing. Is there a reason behind what I’m doing? And did it work? I wish there was more. In cases where teachers felt isolated and disconnected from district colleagues, they often reported relying on other self-contained classroom teachers for support and consultation, rather than resources in their district or from the research literature: When you’re in an EBD class you can get pretty isolated . . . but the other beauty of being in an EBD room is you have other adults in the room that you can talk to, or they can have other ideas, or you can call other teachers. (EBD Teacher, District B) Resources and Tools Related to EBP District commitments to use of EBPs in the classroom were in many cases accompanied by allocation of both material and conceptual resources. The resources and supports most often cited by both administrators and teachers in this con- nection were focused on curriculum materials: Susan, who is our Special Ed curriculum developer, and Louisa, who’s our curriculum facilitator . . . they recognize that we’ve shifted practice to a really research-based practice . . .
- 66. We never really did this [before] we just bought books and Hudson et al. 33 stuff. And I said, “Well, I don’t operate that way. We’re going to shift practice and I’m going to help you” . . . and she has actually been very, very successful at reaching out and capturing the attention of folks, authors that publish . . . and some other materials and some other research and then digging deep. (Special Education Director, District A) I think there’s something really powerful about having that scope and sequence and that repetition that gradually builds on itself. Yeah so instead of me trying to create it as I go, having that research-based program, and of course I’m going to see if it’s not working, then I’m flexible to change it, but I’m going to have a good base to at least start with. (Resource Room Teacher, District B) While district curriculum resources (which were often assumed to be evidence-based) were important tools for many resource room teachers we interviewed, both teachers and administrators expressed frustration about what they viewed as a paucity of evidence-based curriculum and instructional resources for students in self-contained pro- grams, particularly those serving students with low-inci- dence disabilities: There’s not a lot of curriculum out there for the self-contained classrooms. So we do have some, some for our more mild self- contained programs, specific reading, writing, math curriculums. But we also made our own library we call it “The Structured Autism Library” . . . it’s a library of materials we have online that we’ve developed ’cause you can’t really pull
- 67. anything off the shelves for those kinds of kids. (Special Education Director, District D) . . . in self-contained settings in Ocean View, I think that I am expected to . . . sort of use Gen Ed assessments, but in Kindergarten they already test out of those, they already fail so miserably at those. I am then the expert because there’s no assessments that assess these kids’ growth so I make my own assessments. (Self-Contained Classroom Teacher, District D) In the context of these perceptions about the lack of relevant evidence-based resources, we found that only a few teach- ers undertook individual efforts to locate and use available research. Those who did often encountered considerable difficulty in locating relevant research resources: If I’m implementing something I’m not so good at then I’ll go do some reading on it. The Autism modules online are helpful. I’d say mostly every time I try and type something in for a problem I’m having without knowing if there is any research on it, I can never find it, hardly ever. (Self-Contained Classroom Teacher, District C) More often, teachers adopted a “progress monitoring” approach to evidence and decision making: “We take what we learn about the kids and we change how we instruct them, so that’s kind of what we do every day . . . based on each kid and their individual performance” (Self-Contained Classroom Teacher, District B). After our examination of each separate element of the system, we analyzed the interactions between elements to understand the transactional, contextual nature of practitio- ners’ understanding of EBPs.
- 68. A Holistic View: Relationships Between People, Tools, and Organizations Our data suggest that the positions practitioners occupied within their schools and districts had considerable influence on their access to useful resources and tools related to EBP. The nature of the tools available to them, in turn, affected practitioner experiences with and beliefs about the value and relevance of EBPs in the context of decisions they were making. Our findings are summarized below in terms of some specific hypotheses regarding the ways in which these dimensions of practice are related to one another. Hypothesis 1: Practitioner beliefs about the value and relevance of EBP are shaped by the affordances and con- straints of the tools and resources they use for decision making. Similar to other researchers (e.g., Boardman et al., 2005; Landrum et al., 2002), we found some skepticism about the practical relevance of research for local decision making across all of the practitioner groups we interviewed. However, we also noted that this view was most prevalent among self-contained classroom teachers and particularly among teachers of students with low-incidence disabilities. In many cases, both teachers and administrators working with students with low-incidence disabilities expressed the belief that research on “kids like ours” did not exist. For example, a Self-Contained Classroom Teacher in District B explained her stance about research and practice this way: Well it’s just that there’s not a lot out there for me and maybe it’s hard to find. I feel like through my multiple programs, I’ve looked at a lot and there’s just not a lot out there. And I know why—this is a small fraction of the population.
- 69. In some cases, teachers in our study described themselves as having access to curriculum tools they considered to be evidence-based for some populations, but inappropriate for the specific students they served. Hypothesis 2: Practitioner access to relevant tools and resources is affected by the position they occupy within the school and the district. The self-contained classroom teachers we interviewed often described themselves as being extremely isolated, and as 34 The Journal of Special Education 50(1) having relatively little access to tools and resources (research studies, evidence-based curriculum, and relevant evidence- based professional development) they viewed as useful for the students they taught. We found that teachers who worked in positions that were relatively close to general education often had access to more tools and resources (evaluation instruments, curriculum guides, professional development) related to EBP, but were also more likely to encounter ten- sions between mandates from general education, and prac- tices they viewed as appropriate for students with special education needs. The effects of organizational position were also mediated by district policies and practices around col- laboration. For example, one district had strategically devel- oped specific organizational policies and practices to support collaboration among their self-contained classroom teachers. One of the teachers in this district commented on the value of these practices as a support for implementation of EBPs: I definitely believe in the PLC (professional learning
- 70. community) model and just sharing ideas and having, taking on new strategies, and monitoring our own use of them. I think that is kind of the future. I think you’re going to get more buy-in, than a sit and get PD session on evidence-based practice. I think its been proven actually, that you just sit and get it and then you don’t have to use it, no one checks in with you to make sure you are using it. So making groups of people accountable (to each other) makes a ton of sense to me. (Self- Contained Classroom Teacher, District B) More often, however, district policies, resources, and sup- ports related to EBP were reported to be focused on curricu- lum and instructional programs for students with high-incidence disabilities. Teachers in self-contained classrooms often found these tools and resources, and the idea of EBP to be of little direct value to their daily work. Hypothesis 3: How practitioners define EBP affects how they interpret the value and relevance of tools and other organizational resources available to them related to EBP. As we explain further later on, most of the teachers and administrators we interviewed defined EBP primarily in terms of prescriptions for practice that were made by exter- nal authorities. Many of these informants were also those who expressed ambivalence, and often outright skepticism, about the value of EBPs for their work. In contrast to this pattern, a few of the practitioners we talked with appeared to have a more nuanced way of defining EBP. In these cases, EBP was defined less as a prescription for practice than as a resource for decisions they would make in the classroom: I think it would be wonderful to be informed of that research, and the best teacher would have all that information, and be
- 71. able to look at the kid, and provide them an opportunity with a program that is research-based and validated and everything, and look at how the child is responding to the program, give it a little bit of time, make sure you’re delivering it with authenticity and the way it’s supposed to be delivered, you know, give it 3–4 weeks, and if it’s not working you need to find something else. (Resource Room Teacher, District B) Discussion Over the last decade, the notion of EBP has become one of the most influential policy constructs in the field of special education. In this study, we sought to improve our under- standing of the ways practitioners define the idea of EBP and interpret its relevance in the contexts of their daily practice. In addition, we hoped to extend previous research by learn- ing more about some of the contextual factors that might influence practitioner views about EBP. To investigate these two issues, we conducted interviews with special education professionals in four local school districts, including those occupying positions as directors of special education, resource room teachers, self-contained classroom teachers of students with emotional and behavioral disabilities, and teachers of students with low-incidence developmental dis- abilities. Our analysis of these data was guided by some gen- eral precepts drawn from sociocultural theory (Chaiklin & Lave, 1993; Vygotsky, 1978), particularly the idea that social practice can be understood as a process in which individuals are continually negotiating ways of participating in collec- tive activity (Nicolini, Gherardi, & Yanow, 2003). We found that the practitioners we interviewed often defined EBP in ways that externalized the locus of authority for what constituted relevant evidence for practice as the results of “studies someone had done.” Ironically, this view