
Recommended
Recommended
More Related Content
Similar to Jails and PrisonsLooking inside total institutionsDefini.docx
Similar to Jails and PrisonsLooking inside total institutionsDefini.docx (10)
More from vrickens
More from vrickens (20)
Recently uploaded
Recently uploaded (20)
Jails and PrisonsLooking inside total institutionsDefini.docx
- 1. Jails and Prisons Looking inside total institutions Definition of total institution Canadian Erving Goffman coined this term He wrote, “A total institution may be defined as a place of residence and work where a large number of like-situated individuals cut off from the wider society for an appreciable period of time together lead an enclosed formally administered round of life (Goffman, 1968: 11). "Total institutions (such as prisons, boarding schools, psychiatric hospitals, concentration camps, etc. ) are distinctive and have much in common" (Goffman, 1968: 15) because, as Goffman points out, they depart from the basic social arrangements in modern western society "that the individual tends to sleep, play and work in different places with different co-participants, under different authorities and without an overall rational plan" (Goffman, 1968: 17). Glimpses inside the total institution It is very difficult to appreciate what life is like in jail or prison so I have selected a few videos, and stories for you Please listen to Ismael Nazario who speaks about his experience in Rikers as a youth https://www.ted.com/talks/ismael_nazario_what_i_learned_as_a _kid_in_jail?language=en#t-671125 Also, please read a piece published by the Marshall project here https://www.themarshallproject.org/2018/07/12/a-day-in-the- life-of-a-prisoner Finally, hear the story of Mr. Melendez who spent 17 years on death row for a crime he did not commit. Now exonerated, he
- 2. has visited UTA and spoken about this experience. He paints a vivid picture of those 17 years here https://www.youtube.com/watch?v=9k6C7ZVhaHE Why is working in prisons important for social workers? Criminal justice system is marked by the confluence of race, class, gender, and inequality in the United States Mass incarceration has been called one the most pressing social problems of our time (Mauer & Chesney-Lind, 2002) The CJ system is fragmented Over 50,000 different agencies responsible Prisons account for the fastest growing segment of government employment (nearly 750,000 people in 2004) Most people are imprisoned for non-violent crimes Remember that Race, Class, Gender Matter African American men disproportionately imprisoned Women account for the fastest growing prison population African American women: 571% increase in 20 years Latinas: 131% increase in 20 years Caucasian women: 75% increase in 20 years More women are incarcerated per capita for drug crimes than men (about 34% of women and 19% of men) 60% of men and 40% of women unemployed at arrest, 1/3 earned less than 5000$ last year. Privatization of prisons – total institutions and turning a profit for shareholders Beck, A.J. (2000). Prisoners in 1999. Washington, DC: Bureau of Justice Statistics; Guerino, P., Harrison, P.M., & Sabol, P.M. (2011). Prisoners in 2010. Washington, DC: Bureau of Justice Statistics. Prisoners in 1999 available online here:
- 3. http://bjs.ojp.usdoj.gov/content/pub/pdf/p99.pdf Private prisons in Texas http://www.texasprisonbidness.org/map https://www.texasobserver.org/private-prison-bubble-bursts/ Draw of Private prisons Lower costs Good investment for stakeholders Cheap labor for big business (IBM, Nortel, Texas Tech, Target, etc.) Address massive increase in carceral population BUT Safety of inmates and guards compromised Incentive to increase carceral population Dodgy ethics Private facilities Pay prisoners less for labor (as little as 17 cents per hour or $20/month) Less rigid hiring practices Higher inmate to guard ratios Not always advantageous to local work force Running Head: UNTREATED ADHD 1
- 4. UNTREATED ADHD 4 Student’s name: Professor’s name: Topic: Institution: Date: Untreated ADHD To solve the problem of untreated ADHD, one solution would be conducting a risk -benefit analysis. Since many families struggle with whether to put their ASHD child under treatment or not, a risk-benefit analysis could greatly help such families take the bold step in putting their child under ADHD treatment. In this case, healthcare professionals engaging parents who are resistant about their child receiving ADHD treatment can, together with the parent, conduct a risk -benefit analysis to weigh the pros and cons of the treatment. When defining the risks, health professionals should focus more on the larger picture, that is, what the child is set to gain with the ADHD medication. The advantage of this solution is that since it is the healthcare professional facilitating the risk-benefit analysis, they can concentrate more on the positive sides of the ADHD medication and focus less on the negative effects of the
- 5. medication, ultimately winning the support of the parent (Rief, 2015). Through a risk -benefit analysis, the chances of persuading a parent to treat their child are high because the healthcare professional gets to emphasize on the medication benefits and how these benefits outweigh the risks associated with ADHD medication. The challenge with this solution is that it might be hard trying to help parents overcome the fears they have about placing their child under ADHD medication. Another challenge is that carrying out a risk -benefit analysis may be a time - consuming process since it requires responding to every detail and question posed to the satisfaction of the parent skeptical about putting their child with ADHD on medication. The second solution would be creating more awareness as an attempt to set the record straight (Wright et al., 2015). In this case, awareness-raising events could be organized to educate members of the society on the importance of seeking early treatment for ADHD, and empower those reluctant to seek treatment to take the initiative. Spreading awareness on ADHD is also aimed at breaking stereotypes and misconceptions linked to ADHD treatment, and to facilitate this, evidence-based information must be used. One advantage with this solution is that there are many platforms that can be used to raise public awareness on ADHD, and so chances of reaching a wider audience, particularly those reluctant to seek treatment, are high. Creating awareness also makes those unaware of ADHD to create connections between the problems in life and ADHD, prompting them to seek medical assistance to find out whether they indeed have ADHD. The challenge of creating awareness is that it needs to be done periodically for it to be more effective. Additionally, with creating awareness, a lot of effort has to be put to ensure that the ADHD message reaches the intended audience. In regards to the risk-benefit analysis, a child or an adolescent’s chances of being placed under treatment are high, and they will eventually get experience improved social relationships with friends’
- 6. family and schoolmates. In regards to creating awareness, an adults living with the condition will be empowered to seek treatment, and this will promote benefits such as increased job performance, and the ability to sustain work and interpersonal relationships. Besides the proposed solutions, another idea would be the wider use of ADHD therapy treatment approaches to prevent the overreliance of ADHD medication. I would also propose the implementation of ADHD education programs in schools to create more awareness of the condition among school goers. References Rief, S. F. (2015). The ADHD book of lists: A practical guide for helping children and teens with attention deficit disorders. John Wiley & Sons. Wright, N., Moldavsky, M., Schneider, J., Chakrabarti, I., Coates, J., Daley, D., ... & Sayal, K. (2015). Practitioner review: pathways to care for ADHD–a systematic review of barriers and facilitators. Journal of Child Psychology and Psychiatry, 56(6), 598-617. PSYC 6393/FPSY 6393/IPSY 6393: Capstone Social Change Walden University was founded on the principle of promoting positive social change. This remains the guiding philosophy as described in the university’s mission and vision statements: Mission Walden University provides a diverse community of career professionals with the opportunity to transform themselves as scholar-practitioners so that they can effect positive social change. Vision Walden University envisions a distinctively different 21st- century learning community where knowledge is judged worthy
- 7. to the degree that it can be applied by its graduates to the immediate solutions of critical societal challenges, thereby advancing the greater global good. Social Change at Walden University Walden University defines positive social change as a deliberate process of creating and applying ideas, strategies, and actions to promote the worth, dignity, and development of individuals, communities, organizations, institutions, cultures, and societies. Positive social change results in the improvement of human and social conditions. This definition of positive social change provides an intellectually comprehensive and socially constructive foundation for the programs, research, professional activities, and products created by the Walden academic community and services offered by Walden’s Center for Social Change. In addition, Walden University supports positive social change through the development of principled, knowledgeable, and ethical scholar-practitioners who are and will become civic and professional role models by advancing the betterment of society. Walden University General Policies and Governance (November 2018) Writing for Social Change in the Capstone Developing a social change implications framing. Remember, these are potential social change implications, so using language like may, might, could, is appropriate and preferred. 1. Begin with your sample (individual or group that is the focus on your Capstone problem). Explain how the results of the capstone will help the specific individuals or group related to your study. 2. Consider whether the same is true for the larger population
- 8. (community or local municipality). Now that you have described how the actual individuals might use this information, think about whether the larger population may see the same results. a. How might the larger population benefit? b. What are the potential outcomes for the larger population if they took action based on your results? 3. Consider a larger benefit to society (state, national, and international). a. If the larger population implements changes, what broader changes might society benefit from (policy, laws, social views). b. These are generally larger scale ideas that have broader implications. 4. Be sure that you tie the potential social change implications to the problem statement. The goal of the capstone is to address the problem. As such students should ensure that potential positive social change implications are related specifically back to the problem. Adapted from: https://academicguides.waldenu.edu/formandstyle/writing/social change © Walden University 2019 PSYC 6393/FPSY 6393/IPSY 6393/DPSY 6393: Capstone
- 9. Problem Solution Preparation Now that you have critically analyzed the problem, the next step is generating a solution. Please review the following steps in creating the problem solution for your identified Capstone problem. Step 1 Identify the goal in developing a solution. Using the evacuation plan problem from the Problem Statement Examples, the goal would be to prevent the Hurricane Katrina disaster from occurring again by creating an effective, well- developed evacuation plan. Step 2 List several possible solutions that you found support for in the scholarly literature. Also, include a possible solution that you created from your own ideas or expertise in this area. This is a short list of possible solutions for the evacuation plan for New Orleans:
- 10. Have emergency management officials trained on a variety of evacuation plans from around the country prior to revising the plan for New Orleans. Develop ways to educate/inform the entire city about the newly revised evacuation plan, including how it works and maps showing where people would go and how they would get there. Develop evacuation plan drills for the city to practice the plan to ensure that it works properly. Step 3 For each possible solution, think about the advantages and disadvantages. Is it a realistic solution? Is it manageable? What are the costs and benefits of the solution? What are the challenges and barriers to the solution? Here is a sample analysis using the example of evacuation drills for the city: This is probably not a realistic plan considering the size of the city. It would be financially costly, as the emergency staff would have to be paid and the National Guard troops alerted. It is probably unmanageable, given that it would require that residents leave their jobs and schools to participate in a drill. Step 4
- 11. Choose one solution that seems most workable for alleviating the problem. Describe the advantages and disadvantages of the solution. What challenges or barriers might occur with this solution? Discuss the potential for social change that could occur if this solution is implemented. Support your problem solution with citations to the research literature. © Walden University 2019 Am J Psychiatry 166:1, January 2009 103 Article ajp.psychiatryonline.org This article is featured in this month’s AJP Audio, is the subject of a CME course (p. 123), and is discussed in an editorial by Dr. Lamb (p. 8).
- 12. Psychiatric Disorders and Repeat Incarcerations: The Revolving Prison Door Jacques Baillargeon, Ph.D. Ingrid A. Binswanger, M.D., M.P.H. Joseph V. Penn, M.D. Brie A. Williams, M.D., M.S. Owen J. Murray, D.O. Objective: A number of legal, social, and political factors over the past 40 years have led to the current epidemic of psy- chiatric disorders in the U.S. prison sys- tem. Although numerous investigations have reported substantially elevated rates of psychiatric disorders among prison in- mates compared with the general popu- lation, it is unclear whether mental illness is a risk factor for multiple episodes of in-
- 13. carceration. The authors examined this association in a retrospective cohort study of the nation’s largest state prison system. Method: The study population included 79,211 inmates who began serving a sen- tence between September 1, 2006, and August 31, 2007. Data on psychiatric dis- orders, demographic characteristics, and history of incarceration for the preceding 6-year period were obtained from state- wide medical information systems and analyzed. Results: Inmates with major psychiatric disorders (major depressive disorder, bi- polar disorders, schizophrenia, and non- schizophrenic psychotic disorders) had substantially increased risks of multiple incarcerations over the 6-year study pe- riod. The greatest increase in risk was ob- served among inmates with bipolar disor- ders, who were 3.3 times more likely to have had four or more previous incarcer-
- 14. ations compared with inmates who had no major psychiatric disorder. Conclusions: Prison inmates with major psychiatric disorders are more likely than those without to have had previous incar- cerations. The authors recommend ex- panding interventions to reduce recidi- vism among mentally ill inmates. They discuss the potential benefits of continu- ity of care reentry programs to help men- tally ill inmates connect with community- based mental health programs at the time of their release, as well as a greater role for mental health courts and other diversion strategies. (Am J Psychiatry 2009; 166:103–109) The epidemic of psychiatric disorders in the U.S. prison system represents a national public health crisis. Epidemiologic studies show that 15%–24% of U.S. inmates have a severe mental illness (1–3), and a recent report by the Bureau of Justice Statistics indicates that half of in- mates—over 1 million individuals—have at least one
- 15. mental health condition (4). Several factors have synergis- tically led to the excess of mental illness in the U.S. correc- tional system. In the late 1960s, with the availability of new antipsychotic medications, a national movement resulted in the mass closing of public mental health hospitals (5–7). Many leaders in the psychiatric community argued that moving patients out of state hospitals and into commu- nity-based outpatient settings represented a humane al- ternative to overcrowded and understaffed institutions. Unfortunately, in most cases, the closing of state hospitals was not accompanied by the promised number of clinics and halfway houses necessary to care for released hospital patients (5–7). In subsequent years, health insurers re- stricted mental health coverage, private hospitals limited enrollment of psychotic patients, and civil commitment laws became more restrictive (5). Additionally, beginning in the 1980s, the “war on drugs,” which led to an increase in drug-related arrests and an emphasis on mandatory and fixed sentencing, resulted in dramatic increases in the proportion of inmates with psychiatric disorders and sub- stance abuse problems (8, 9). All of these factors have cul- minated in a revolving-door phenomenon in which many mentally ill people move continuously between homeless- ness and the criminal justice system (5, 10).
- 16. Despite the magnitude of this problem, few studies have examined the association between psychiatric disorders and recidivism in correctional populations (11–13). Recid- ivism is generally defined as a relapse into previous crimi- nal behavior; in most published studies, it is operationally defined as a repeat arrest or incarceration. These studies, which have focused on relatively small and specific sub- groups of the correctional population, have found little or no association between psychiatric disorders and the risk of having a single repeat incarceration. To our knowledge, no study has examined the association of psychiatric dis- orders with multiple episodes of incarceration. This gap in 104 Am J Psychiatry 166:1, January 2009 PSYCHIATRIC DISORDERS AND REPEAT INCARCERATIONS ajp.psychiatryonline.org the research is noteworthy given the cyclical nature of in- carceration and homelessness among many impoverished
- 17. mentally ill people in the United States (5, 10). In this study, we examined whether inmates with one of four types of major psychiatric disorders had an increased risk of having multiple episodes of incarceration in the Texas Department of Criminal Justice (TDCJ) prison system, the largest state correctional system in the United States (14). Method Design and Study Sample This was a retrospective cohort study of all TDCJ inmates (N= 79,211) who began serving sentences between September 1, 2006, and August 31, 2007, in any of TDCJ’s 116 facilities throughout the state. The inmates’ history of previous TDCJ incarcerations was determined by examining a comprehensive electronic database containing all TDCJ incarceration records from September 1, 2000, through August 31, 2006. A previous incarceration was de- fined as an incarceration resulting from a distinct criminal of- fense; previous incarcerations resulting from parole violations were not included in our analysis. All members of the study co- hort underwent standard medical and psychiatric examinations
- 18. during the intake process. This evaluation lasted approximately 60 minutes and consisted of a detailed medical history, a mental health screening, a physical examination, and a number of labo- ratory tests. The study was reviewed and approved by the Univer- sity of Texas Medical Branch Institutional Review Board. Measures The study was designed to compare the prevalence of having multiple episodes of incarceration among inmates with any of four types of major psychiatric disorders: major depressive disor- der, bipolar disorders, schizophrenia, and nonschizophrenic psy- chotic disorders. Nonschizophrenic psychotic disorders included schizoaffective disorder, delusional disorder, substance-induced psychosis, and psychotic disorder not otherwise specified. The mental health screening at the time of the intake evaluation was conducted in a standardized fashion across all prison sites by mental health nurses or mental health professionals. The screen- ing consisted of a standardized diagnostic interview and included assessment of the following: display of symptoms of psychiatric disease; history of mental health treatment; current suicidal ide- ation; prior suicidal gestures; display of unusual behavior;
- 19. affec- tive distress; and unusual nature of criminal offense. The purpose of the intake screening was to determine whether an inmate should be referred for a formal mental health evaluation. If a re- ferral was made, the evaluation was conducted by master’s-level mental health professionals using a DSM-IV-guided interview structure. A diagnosis of a psychiatric disorder established during this evaluation was based on DSM-IV criteria and recorded in the inmate’s electronic medical record. All incoming inmates who had one of the four types of major psychiatric disorders under study, who reported a history of treatment with psychotropic medication, or who appeared to require such treatment were sub- sequently referred to a staff psychiatrist or a psychiatric midlevel practitioner for treatment. Diagnoses that were made or con- firmed by psychiatric providers were also based on DSM-IV crite- ria. Approximately 20% of all inmates were referred for psychiat- r i c e v a l u a t i o n d u r i n g th e i r i n c a rc e ra ti o n . A l l p s y c h i a t r i c
- 20. diagnoses used in the analyses in this study were ascertained dur- ing the period from September 2006 through August 2007. All demographic data (age, race/ethnicity, and gender) were based on inmate self-reports and maintained in a systemwide electronic medical record that is routinely updated to ensure that the information reflects the inmates’ current health status. Infor- mation on correctional characteristics (criminal offense classifi- cation and length of prison sentence) was maintained in a sepa- rate electronic database. Criminal offense classification was based on the National Criminal Information Center criminal of- fense codes associated with the inmates’ current sentence. In- mates who had at least one violent criminal offense (i.e., homi- cide, kidnapping, sexual assault, robbery assault, and terrorism) were classified as violent; inmates who had no such criminal of- fenses were classified as nonviolent. The two electronic data sets were linked using a common numeric identification variable. Statistical Analyses
- 21. All statistical analyses were performed with SAS, version 8 (SAS Institute, Cary, N.C.). Logistic regression analysis was used to ex- amine differences in multiple episodes of incarceration across the subgroups and to calculate adjusted prevalence odds ratios and corresponding 95% confidence intervals (CIs). All logistic re- gression models were adjusted for age, gender, race/ethnicity, criminal offense classification, and length of current prison sen- tence. Information on at least one of the aforementioned demo- graphic or correctional variables was unavailable in <1% of the study population; inmates with missing data were excluded from the analysis. Results Of the 71,333 inmates in the study cohort who did not have any of the four major types of psychiatric disorders, the vast majority were male (87.2%), were under 50 years old (90.1%), were currently incarcerated for a nonviolent offense (79.2%), had no history of a violent offense during the 2000–2006 period (79.4%), and had a current prison sentence of less than 2 years (60.1%). The three racial/eth- nic groups were distributed fairly evenly: 34.3% were non-
- 22. Hispanic Caucasian, 30.0% were Hispanic Caucasian, and 35.7% were African American. A total of 7,878 inmates were diagnosed with major depressive disorder, a bipolar disor- der, schizophrenia, or a nonschizophrenic psychotic disor- der. There was substantial variation in several demo- graphic characteristics according to the psychiatric disorders under study (Table 1). Among inmates diagnosed with major depressive disorder and bipolar disorders, fe- males and non-Hispanic Caucasians were overrepresented and Hispanics and African Americans were underrepre- sented. Among inmates with schizophrenia and non- schizophrenic psychotic disorders, African Americans, in- mates age 50 or older, and inmates who had violent offense records (current or previous) were overrepresented. The percentage of specific criminal offenses was calcu- lated according to the four major types of psychiatric dis- orders (Table 2). Assessment of the major violent offenses showed that, in comparison with inmates who had no psy- chiatric disorder, those who had any psychiatric disorder, a bipolar disorder, schizophrenia, or a nonschizophrenic psychotic disorder had higher rates of assault; inmates who had schizophrenia or a nonschizophrenic psychotic
- 23. Am J Psychiatry 166:1, January 2009 105 BAILLARGEON, BINSWANGER, PENN, ET AL. ajp.psychiatryonline.org disorder had higher rates of homicide; and inmates who had any psychiatric disorder, schizophrenia, or a non- schizophrenic psychotic disorder had higher rates of rob- bery. Assessment of major nonviolent offenses showed that, in comparison with inmates who had no psychiatric disorder, those who had any psychiatric disorder, major depressive disorder, schizophrenia, or a nonschizophrenic psychotic disorder had lower rates of driving under the in- fluence; inmates who had schizophrenia or a nonschizo- phrenic psychotic disorder had higher rates of drug pos- session; and inmates in all major psychiatric disorder categories had higher rates of property offenses. The prevalence of having previous incarcerations was calculated for inmates with each of the four major types of psychiatric disorders, using four different threshold val- ues: ≥1, ≥2, ≥3, and ≥4 incarcerations (Table 3). Odds ra- tios, adjusted for gender, age, race, current criminal of-
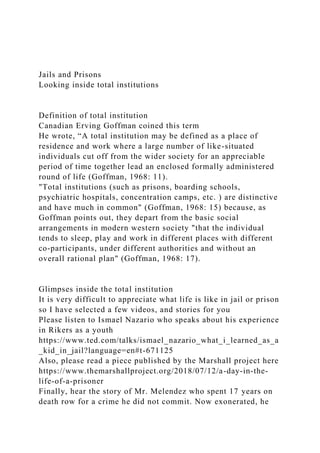
- 24. fense classification (violent versus nonviolent), and length of current sentence, were then calculated to assess the risk of each threshold value among each of the four groups of psychiatric disorders. For three of the four categories of psychiatric disorders (bipolar disorders, schizophrenia, nonschizophrenic psychotic disorders), the risk of having multiple incarcerations increased in a stepwise fashion according to the threshold value (Figure 1). For inmates with major depressive disorder, the risk of having previous incarcerations remained relatively stable across all four threshold values. Discussion Our study showed that Texas prison inmates with major psychiatric disorders were far more likely to have had pre- vious incarcerations compared with inmates without a serious mental illness. For three of the categories of psy- chiatric disorders under study (bipolar disorders, schizo- phrenia, and nonschizophrenic psychotic disorders), this risk increased in a stepwise fashion according to the threshold value for number of incarcerations. The risk of having four or more incarcerations in the 6-year study pe- riod was particularly high for inmates with a bipolar disor-
- 25. der. In general, these findings suggest a substantially heightened risk of recidivism among released inmates with mental illness. As a result of the limited availability of TABLE 1. Percent Distribution of Demographic and Criminal Offense Characteristics of the Study Population, by Psychiatric Disorder Characteristic No Psychiatric Disorder (N=71,333) Any Psychiatric Disorder (N=7,878) Major Depressive Disorder (N=3,252)
- 26. Bipolar Disorders (N=2,402) Schizophrenia (N=849) Nonschizophrenic Psychotic Disorders (N=1,375) Male 87.2 71.4 61.3 70.7 91.5 84.1 Race/ethnicity Non-Hispanic Caucasian 34.3 51.7 53.5 69.2 24.5 33.6 Hispanic Caucasian 30.0 15.6 16.8 12.6 15.6 17.9 African American 35.7 32.7 29.7 18.1 60.0 48.5 Age (years) 16–29 40.5 26.5 25.8 31.1 18.1 25.1 30–49 49.6 62.5 62.0 62.5 62.3 63.6 ≥50 9.8 11.0 12.1 6.4 19.6 11.3 Current criminal offense Violent 19.8 20.6 17.9 19.4 26.6 25.3
- 27. Nonviolent 79.2 79.4 82.1 80.6 73.4 74.7 Previous criminal offense Violent 19.6 22.3 19.4 19.6 29.6 27.9 Nonviolent 79.4 77.7 80.6 80.4 70.4 72.1 Current sentence length <2 years 74.6 73.6 73.7 74.5 74.5 73.5 ≥2 years 25.3 24.6 26.3 25.4 25.5 26.5 TABLE 2. Percent Distribution of Specific Criminal Offenses of the Study Population, by Psychiatric Disorder Offense No Psychiatric Disorder (N=71,333) Any Psychiatric Disorder (N=7,878)
- 28. Major Depressive Disorder (N=3,252) Bipolar Disorders (N=2,402) Schizophrenia (N=849) Nonschizophrenic Psychotic Disorders (N=1,375) Violent offenses Assault 13.0 16.4a 14.0 16.0a 21.7a 19.7a Homicide 1.8 2.3 1.9 1.8 3.8 a 3.1a Robbery 8.6 9.7a 8.2 8.1 12.1a 14.6a Nonviolent offenses
- 29. Driving under the influence 10.8 8.8b 9.3b 10.0 4.8b 8.1b Drug possession 8.6 8.3 7.2 7.1 12.4a 10.5a Drug delivery (dealing) 43.3 42.7 42.9 42.1 42.8 42.9 Property offenses 43.2 52.6a 50.5a 54.5a 53.6a 53.7a a Exhibited a statistically significantly higher percentage of the criminal offense compared with inmates in the “no psychiatric disorder” group, as determined by assessing overlap of 95% confidence intervals. b Exhibited a statistically significantly lower percentage of the criminal offense compared with inmates in the “no psychiatric disorder” group, as determined by assessing overlap of 95% confidence intervals. 106 Am J Psychiatry 166:1, January 2009 PSYCHIATRIC DISORDERS AND REPEAT INCARCERATIONS ajp.psychiatryonline.org
- 30. community-based mental health services, mass downsiz- ing of state psychiatric institutions, and a legal system with a limited capacity to discern underlying mental health problems, many people with serious mental illness move continuously between crisis hospitalization, home- lessness, and the criminal justice system (10, 15). To our knowledge, this is the first study to examine the associa- tion of psychiatric disorders and multiple episodes of in- carceration in an entire state prison population. Only a handful of studies (12, 13, 16, 17) involving cor- rectional populations have examined the association be- tween psychiatric disorders and the risk of having a single reincarceration. In contrast to our findings, each of these investigations found that inmates with mental disorders exhibited either comparable (16, 17) or lower (12, 13) rein- carceration rates for both violent and nonviolent offenses in comparison with inmates without psychiatric disor- ders. However, a direct comparison of our results with those of earlier studies is of limited value because of differ- ences in sample sizes and methods used to assess psychi- atric disorders and recidivism. Feder (16) examined rein- carceration rates among 547 inmates released from the New York State prison system in 1982 and 1983. Lovell et
- 31. al. (17) examined reincarceration rates among 337 men- tally ill inmates released from Washington State prisons in 1996 and 1997. Teplin et al. (12) assessed violent repeat of- fenses among 728 male jail detainees in Chicago in 1983 and 1984. Porporino and Motiuk (13) examined all repeat offenses among 36 Canadian inmates with a major psy- chotic disorder and 36 comparison inmates with no psy- chiatric disorder. In each of these studies, findings of com- parable or lower reincarceration rates among mentally ill inmates may be due to several factors. For example, in- mates with psychiatric disorders are reported to stay in prison longer than others charged with similar crimes (18). The average time served for U.S. inmates with mental il lness is 103 months (8.6 years), compared with 88 months (7.3 years) for other prisoners (19). Another possi- ble factor may be geographic differences in the efficacy of community-based mental health programs and prison discharge planning programs in preventing criminal re- cidivism in former inmates (20). Our investigation’s novel findings may be attributable to a number of factors. One possibility is that the criminal justice policies of Texas result in higher rates of incarcera- tion among persons with mental illness. Another is that
- 32. community-based mental health systems in Texas may have been less effective in diverting persons with severe mental illness from the criminal justice system. However, Texas does have a state-sponsored continuity of care pro- gram that links inmates with serious mental illness who are about to be released to treatment resources in their home communities, including halfway houses and outpa- tient clinics. The program also provides inmates with a 10- day supply of their prescribed psychotropic medications. Unfortunately, few data on inmates’ participation in this program are currently available. Several limitations should be considered in interpreting our study. We examined only incarcerations within the Texas prison system. If an inmate in our study population was previously incarcerated in another state, the episode was not included in our analysis. However, given the large geographic size of Texas and the limited mobility of our study population, it is unlikely that a substantial propor- tion of inmates had been incarcerated in another state’s prison system. Second, because relatively less severe psy- chiatric disorders such as anxiety disorders and axis II dis- orders are not rigorously evaluated in the TDCJ, during ei- ther the initial mental health screening or subsequent medical encounters, we restricted our analyses to four
- 33. broad categories of severe psychiatric disorders. Addition- ally, information about a prisoner’s history of substance abuse is maintained in a separate, confidential TDCJ data- base that was not available for analysis. Thus, our ability to assess the extent to which either less severe psychiatric conditions or substance use disorders contributed, either independently or comorbidly, to repeat incarcerations was limited. Third, this investigation was subject to the se- lection biases associated with most retrospective study designs. Specifically, inmates who were incarcerated mul- tiple times may have had a greater probability of being di- agnosed with a serious mental illness. This bias was prob- ably mi ni mized by th e s t andard i zed me nt al healt h evaluation used at intake and by our decision to restrict our analysis to four categories of the most severe psychiat- ric disorders. A fourth limitation of our study was that because of in- complete access to historical incarceration data, we could TABLE 3. Risk of Previous Incarcerations Among Inmates, by Presence of a Psychiatric Disordera ≥1 Incarceration ≥2 Incarcerations ≥3 Incarcerations ≥4 Incarcerations
- 34. Disorder % Odds Ratio 95% CI % Odds Ratio 95% CI % Odds Ratio 95% CI % Odds Ratio 95% CI No major psychiatric disorder 38.7 Ref 12.2 Ref 3.6 Ref 1.1 Ref Any major psychiatric disorder 50.7 1.7 1.6–1.8 20.1 2.0 1.8– 2.4 7.0 2.1 1.9–2.4 2.7 2.4 2.1–2.9 Major depressive disorder 48.5 1.5 1.4–1.6 17.9 1.5 1.4–1.7 5.5 1.5 1.4–1.8 2.0 1.6 1.3–2.1 Bipolar disorders 50.9 1.7 1.6–1.9 20.9 2.1 1.9–2.4 8.0 2.6 2.2– 3.1 3.3 3.3 2.6–4.2 Schizophrenia 51.2 1.4 1.2–1.6 19.7 1.5 1.2–1.8 6.8 1.6 1.2–2.1 2.6 2.0 1.2–3.0 Nonschizophrenic psychotic disorders 54.8 1.8 1.6–2.0 23.9 2.1 1.8–2.4 8.7 2.2 1.8–2.7 3.2 2.4 1.7–3.5
- 35. a Odds ratios were adjusted for gender, age, race, current and previous violent criminal offense classification, current and previous drug-related criminal offense classification, and length of current sentence. Am J Psychiatry 166:1, January 2009 107 BAILLARGEON, BINSWANGER, PENN, ET AL. ajp.psychiatryonline.org not fully examine the extent to which the duration of pre- vious incarcerations may have contributed to differential reincarceration rates between inmates with and without these mental illnesses over the 2000–2006 study period. Although it is possible that inmates with psychiatric disor- ders receive shorter sentences and therefore have greater opportunities to commit new criminal offenses and ulti- mately to be reincarcerated, this scenario is not supported by previous studies, which have consistently shown that mentally ill persons receive longer prison sentences and have a reduced likelihood of early parole compared with
- 36. those who are not mentally ill (13, 19). These results are consistent with our own findings that TDCJ inmates with psychiatric disorders had a longer mean current prison sentence and were more likely than other inmates to be currently incarcerated for a violent crime. Assuming that these two variables would serve as reasonable proxies for previous prison sentence length, we adjusted for both cur- rent prison sentence length and current criminal offense classification in all statistical models and found that their inclusion in the models had only a minimal effect on the outcome of our analyses. Finally, our findings are highly dependent on the reliability and validity of the screening measures, the diagnoses of mental health professionals, and the accuracy of data entry into the electronic medical record. Although TDCJ has policies of universal and stan- dardized medical screening of all inmates at intake, as well as standardized and validated data entry procedures, it is possible that some inmates were misclassified or misdiag- nosed and that some data were entered incorrectly. Despite these limitations, this is the first study to exam- ine the association between major psychiatric disorders and multiple episodes of incarceration within an entire state prison population. Because this investigation was carried out in the nation’s largest state prison system,
- 37. these findings have a high degree of statistical power and are likely to be generalizable to other U.S. prison systems. It is important to recognize, however, that inmates with mental illness represent a small and distinct segment of the broader population of mentally ill adults in the United States and that the overall contribution of mental illness to criminal activity in our society is small (21). The results of our study highlight the need to pursue al- ternatives to incarceration of persons with severe mental illness. One of the most promising alternatives is the di- version model, designed to prevent or minimize law en- forcement detention of the nonviolent mentally ill (22, 23). Based on a foundation of extensive interagency collabora- tion between mental health, law enforcement, and crimi- nal justice systems, the model draws on a wide range of strategies to divert persons with severe mental illness to appropriate community-based mental health services in lieu of incarceration (15, 24). There are two major types of diversion programs. Pre- booking programs, which are designed to resolve psychi- atric emergencies without resorting to arrest, generally are based on formal liaisons between law enforcement and mental health personnel (23, 25). An example is the crisis
- 38. intervention team, which utilizes specially trained police officers to redirect individuals with mental illness to treat- FIGURE 1. Risk of Previous Incarcerations Among Texas Prison Inmates, by Presence of a Psychiatric Disorder 5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5
- 40. 5 % C I) Any Major Psychiatric Disorder Major Depressive Disorder Bipolar Disorder Schizophrenia Nonschizophrenic Psychotic Disorder Psychiatric Disorders ≥1 Incarceration ≥2 Incarcerations ≥3 Incarcerations ≥4 Incarcerations
- 41. 108 Am J Psychiatry 166:1, January 2009 PSYCHIATRIC DISORDERS AND REPEAT INCARCERATIONS ajp.psychiatryonline.org ment instead of the judicial system (22). Preliminary data suggest that the crisis intervention team program is asso- ciated with lower arrest rates and criminal justice costs than other pre- and postdiversion programs (22). Postbooking programs, as the term implies, attempt to divert mentally ill offenders to community-based services after they have been arrested. In contrast to prebooking programs, the criminal justice system plays a major role in postbooking diversion (26). One particularly promising postbooking program is the mental health court, which was designed to divert nonviolent mentally ill individuals from jails and prisons into closely supervised treatment programs (27, 28). The number of mental health courts in the United States has increased from two in 1997 to ap- proximately 120 today (27). Unlike traditional courts, mental health courts have therapeutic goals, such as in- creasing treatment adherence, and they are presided over
- 42. by designated judges (18, 27). Preliminary evidence indi- cates that participation in a mental health court is associ- ated with longer periods without criminal recidivism (18). Another emerging diversion strategy is the forensic asser- tive community treatment model, which relies on 24-hour mobile services and comprehensive outreach modalities, such as mental health and addiction treatment, transpor- tation, economic assistance, and vocational training (24). In addition to diversion strategies, the implementation or expansion of discharge planning or continuity of care programs for mentally ill inmates who are about to be re- leased appears warranted. Ideally, such programs should link released inmates with long-term, community-based outpatient services to help them manage their mental health problems and reduce their risk of recidivism. Be- sides providing outpatient treatment, there is evidence suggesting that community-based mental health pro- grams should make efforts to ensure that ex-inmates have access to acute psychiatric inpatient treatment for an ap- propriate duration. For example, one study (29) found that hospitalizations that are too brief may fail to stabilize es- calating psychiatric symptoms and increase the risk of criminal recidivism. Other studies have shown that co- morbid substance use among persons with mental illness
- 43. also increases the risk of reincarceration (29, 30), suggest- ing that the inclusion of drug and alcohol screening and treatment in community settings may help reduce the rate of recidivism among mentally ill persons (29). Finally, a substantial proportion of inmates with mental illness are incarcerated for violent crimes (20%–25% in our study), especially felony offenses. Because these individu- als are generally ineligible for diversion programs, consid- eration should be given to the development of alternative correctional facilities that would provide an appropriate clinical environment, including expanded opportunities for monitoring and treatment, for inmates suffering from severe mental illness (31, 32). A recent study by the Pew Center on the States esti- mated that, for the first time in U.S. history, more than 1 in 100 adults are confined in an American jail or prison at any given time (14). This striking statistic does not reflect a parallel increase in crime; rather, it is a culmination of criminal justice policies that send more lawbreakers to prison for longer periods. Although the costs of incarcera- tion have increased dramatically, little progress has been made in reducing the rates of recidivism and reincarcera-
- 44. tion, particularly among inmates with mental illness (14). Hence, our finding that inmates with psychiatric disorders have an increased risk of having multiple incarcerations has important policy implications. Addressing this public health crisis adequately will require the continued devel- opment of novel and integrated interventions, such as mental health courts, continuity of care programs, and the development of specialized correctional mental health fa- cilities. Given the scale and complexity of this problem, it is likely that a coordinated effort among criminal justice, mental health, and public health systems will be neces- sary to reduce the widespread criminalization of the men- tally ill in America. Received March 20, 2008; revision received May 30, 2008; ac- cepted July 14, 2008 (doi: 10.1176/appi.ajp.2008.08030416). From the Department of Preventive Medicine and Community Health and the Correctional Managed Care Program, University of Texas Medical Branch, Galveston; Department of Medicine, University of Colorado Denver, Aurora; and the Department of Medicine, University of Cali-
- 45. fornia at San Francisco. Address correspondence and reprint re- quests to Dr. Baillargeon, Department of Preventive Medicine and Community Health, University of Texas Medical Branch, 301 Univer- sity Blvd., Galveston, TX 77555; [email protected] (e-mail). All authors report no competing interests. The authors thank Leonard Pechacek for his editorial assistance. References 1. Teplin LA, Abram KM, McClelland GM: Prevalence of psychiatric disorders among incarcerated women, I: pretrial jail detainees. Arch Gen Psychiatry 1996; 53:505–512 2. Diamond PM, Wang EW, Holzer CE III, Thomas C, des Anges C: The prevalence of mental illness in prison. Adm Policy Ment Health 2001; 29:21–40 3. National Commission on Correctional Health Care: The Health Status of Soon-to-Be-Released Inmates: A Report to Congress.
- 46. Chicago, National Commission on Correctional Health Care, 2002 4. James DJ, Glaze LE: Mental Health Problems of Prison and Jail Inmates. Bureau of Justice Statistics Special Report, NCJ 213600. Washington, DC, US Department of Justice, Sept 2006. http://www.ojp.usdoj.gov/bjs/pub/pdf/mhppji.pdf 5. Butterfield F: Asylums behind bars: a special report; prisons re- place hospitals for the nation’s mentally ill. New York Times, March 5, 1998 6. Kinsler PJ, Saxman A: Traumatized offenders: don’t look now, but your jail’s also your mental health center. J Trauma Disso- ciation 2007; 8:81–95 7. Lamb HR, Bachrach LL: Some perspectives on deinstitutional- ization. Psychiatr Serv 2001; 52:1039–1045 8. Boutwell A, Rich JD: HIV infection behind bars. Clin Infect Dis
- 47. 2004; 38:1761–1763 9. Lurigio AJ, Swartz JA: Changing the contours of the criminal jus- tice system to meet the needs of persons with serious mental illness, in Policies, Processes, and Decisions of the Criminal Jus- Am J Psychiatry 166:1, January 2009 109 BAILLARGEON, BINSWANGER, PENN, ET AL. ajp.psychiatryonline.org tice System. Edited by Horney J. Washington, DC, Department of Justice, 2000, pp 45–108 10. Hoge SK: Providing transition and outpatient services to men- tally ill released from correctional institutions, in Public Health Behind Bars: From Prisons to Communities. Edited by Greifin- ger RB. Dobbs Ferry, NY, Springer, 2007, pp 461–477
- 48. 11. Putkonen H, Komulainen EJ, Virkkunen M, Eronen M, Lönn- qvist J: Risk of repeat offending among violent female offend- ers with psychotic and personality disorders. Am J Psychiatry 2003; 160:947–951 12. Teplin LA, Abram KM, McClelland GM: Does psychiatric disor- der predict violent crime among released jail detainees? a six- year longitudinal study. Am Psychol 1994; 49:335–342 13. Porporino FJ, Motiuk LL: The prison careers of mentally disor- dered offenders. Int J Law Psychiatry 1995; 18:29–44 14. Pew Center on the States: One in 100: Behind Bars in America 2008. Washington, DC, Pew Charitable Trusts, 2008. http:// www.pewcenteronthestates.org/report_detail.aspx?id=35904 15. Kanapaux W: Criminal Justice Primer for State Mental Health Agencies. Alexandria, VA, National Association of State Mental Health Program Directors and National Technical Assistance Center for State Mental Health Planning , 2002. http://
- 49. www.nasmhpd.org/general_files/publications/ntac_pubs/ reports/Primer.pdf 16. Feder L: A comparison of the community adjustment of men- tally ill offenders with those from the general prison popula- tion. Law Hum Behav 1991; 15:477–493 17. Lovell D, Gagliardi GJ, Peterson PD: Recidivism and use of ser- vices among persons with mental illness after release from prison. Psychiatr Serv 2002; 53:1290–1296 18. McNiel DE, Binder RL: Effectiveness of a mental health court in reducing criminal recidivism and violence. Am J Psychiatry 2007; 164:1395–1403 19. Ditton PM: Mental Health and Treatment of Inmates and Pro- bationers. Bureau of Justice Statistics Special Report, NCJ 172211. Washington, DC, US Department of Justice, July 1999. http://www.ojp.usdoj.gov/bjs/pub/pdf/mhtip.pdf 20. Bonta J, Law M, Hanson K: The prediction of criminal and
- 50. vio- lent recidivism among mentally disordered offenders: a meta- analysis. Psychol Bull 1998; 123:123–142 21. Filley CM, Price BH, Nell V, Antoinette T, Pincus J, Bresnahan JF, Pincus JH, Gelbort MM, Weissberg M, Kelly JP: Toward an un- derstanding of violence: neurobehavioral aspects of unwar- ranted physical aggression: Aspen Neurobehavioral Confer- ence consensus statement. Neuropsychiatry Neuropsychol Behav Neurol 2001; 14:1–14 22. Compton MT, Bahora M, Watson AC, Oliva JR: A comprehensive review of extant research on crisis intervention team (CIT) pro- grams. J Am Acad Psychiatry Law 2008; 36:47–55 23. Steadman HJ, Morris SM, Dennis DL: The diversion of mentally ill persons from jails to community-based services: a profile of programs. Am J Public Health 1995; 85:1630–1635 24. Lamberti JS, Weisman R, Faden DI: Forensic assertive commu-
- 51. nity treatment: preventing incarceration of adults with severe mental illness. Psychiatr Serv 2004; 55:1285–1293 25. Lamb HR, Weinberger LE, DeCuir WJ: The police and mental health. Psychiatr Serv 2002; 53:1266–1271 26. Draine J, Solomon P: Describing and evaluating jail diversion services for persons with serious mental illness. Psychiatr Serv 1999; 50:56–61 27. Kuehn BM: Mental health courts show promise. JAMA 2007; 297:1641–1643 28. Thompson M, Osher F, Tomasini-Joshi D: Improving Responses to People With Mental Illness: The Essential Elements of a Men- tal Health Court. New York, Council of State Governments Jus- tice Center, 2007 29. Quanbeck CD, Stone DC, McDermott BE, Boone K, Scott CL,
- 52. Frye MA: Relationship between criminal arrest and community treatment history among patients with bipolar disorder. Psy- chiatr Serv 2005; 56:847–852 30. Hartwell SW: Comparison of offenders with mental illness only and offenders with dual diagnoses. Psychiatr Serv 2004; 55: 145–150 31. Daigle MS, Daniel AE, Dear GE, Frottier P, Hayes LM, Kerhof A, Konrad N, Liebling A, Sarchiapone M: Preventing suicide in prisons, part II: international comparisons of suicide preven- tion services in correctional facilities. Crisis 2007; 28:122–130 32. Konrad N, Daigle MS, Daniel AE, Dear GE, Frottier P, Hayes LM, Kerkhof A, Liebling A, Sarchiapone M: Preventing suicide in prisons, part I: recommendations from the International Asso- ciation for Suicide Prevention Task Force on Suicide in Prisons. Crisis 2007; 28:113–121 Mental Health and Incarcerated People
- 53. Overview of the problem Carceral institutions are largest providers of mental health care 3 times as many SMI in jails and prisons than hospitals Some estimates state more than 50% of incarcerated individuals (and 70% of women) qualify for a mental health diagnosis (Fisher et al, 2014; Gonzalez et al, 2014) 16% of inmates have SMI, about as many have experienced homelessness prior to arrest (Fisher et al 2014). 30-40% of people with SMI have been incarcerated (Fisher et al, 2014) Woefully inadequate care – symptoms worsen with incarceration MH prisoners 2-3 times more expensive More likely to be placed in solitary confinement “In historical perspective, we have returned to the early nineteenth century, when mentally ill persons filled our jails and prisons. At that time, a reform movement, sparked by Dorothea Dix, led to a more humane treatment of mentally ill
- 54. persons. For over a hundred years, mentally ill individuals were treated in hospitals. We have now returned to the conditions of the 1840s by putting large numbers of mentally ill persons back into jails and prisons.” (Torrey et al., 2010) Kevin DeMott 19 years old held in adult prison Diagnosed bipolar disorder 4 months solitary confinement for throwing things off balcony, breaking lightbulbs for self-harm, suicidal behaviors NAMI: Criminalization of “crisis proportions” The National Alliance on Mental Illness warned the U.S. Senate Judiciary Committee in 2016 that criminalization of
- 55. people living with mental illness has reached "crisis proportions“ They called for support of federal, state and local reforms to overcome failings in both the mental health care and criminal justice systems. How does criminalization of SMI people happen? Deinstitutionalization – when asylums were emptied, the needed community based services did not appear, and eventually led to people with serious and persistent mental health problems being swept off the streets by the police Contributing factors include: Homelessness Substance use Increased police contact with broken windows policing policies Revolving door of lack of/absence of treatment – homeless and using – swept off streets by police – stress of jail – release ….repeat Deinstitutionalization Began in the 1960’s. Let’s consider an example from Michigan 1987-2003: 75% of Michigan’s psychiatric facilities closed
- 56. 1955: 1 psychiatric bed for every 300 Americans 2005: 1 psychiatric bed for every 3000 Americans Exacerbated by Institutes for Mental diseases (IMD) exclusion (part of social securities act) Community care fell far short Increased homelessness drug and alcohol use as self-medication (for underlying MI and stress of streets) Police contact Behaviors that frequently accompany mental health problems lead to charges of trespassing, indecent exposure, resisting arrest, minor assault, property damage, etc. Disorderly conduct leads to people being labelled “disordered accused” 1 in 4 police shootings are people with SMI But this is not only a police problem, people with mental health problems often find that CJ involvement exacerbates their underlying reason for CJ contact – their mental health issues
- 57. Effects of Imprisonment isolation from families and social networks austere surroundings, loss of privacy and poor physical and hygienic conditions aggression, bullying, fear, suspicion and the attitudes of unsympathetic and uninformed staff lack of purposeful activity, of personal control, of power to act and loss of identity; pressure to escape or to take drugs shame and stigmatization uncertainty, particularly among remand prisoners, and concern about re-integration into the outside world. Women Inmates and Mental Health Female inmates had higher rates of mental health problems than male inmates 73 percent of females versus of 55 percent of males in state prisons.( Mental Health Problems of Prison and Jail Inmates, Published September, 2006 Bureau of Justice Statistics, US Department of Justice. Note: Based on self report data, not necessarily a formal diagnosis).
- 58. Women and Trauma Sexual Abuse: 57% of females report abuse before admission to state prison versus 16.1 percent of males. 39 % of female state prison inmates report that they were sexually abused before admission to state prison versus 5.8 percent of males. (Prior Abuse Reported by Inmates and Probationers, Published in April, 1999. Bureau of Justice Statistics, US Department of Justice). Physical or Sexual Violence: Nearly 6 in 10 women in state prisons had experienced physical or sexual abuse in the past. 69 % reported that the assault occurred before age 18.( Women Offenders, Published December 1999, Bureau of Justice Statistics, US Department of Justice). Compare suicide rates Rates of suicide for local jail inmates and U.S. residents, per 100,000
- 59. Suicide is leading cause of death in jails More than a third — 34 percent — of all inmate deaths at local jails are self-inflicted, and the rate is increasing (BJS, 2015 report) 7 times higher in jails than prisons (BJS, 2015 report) face a first-time “shock of confinement”; they are stripped of their job, housing, and basic sense of normalcy. Many suicide before they have been convicted at all. Voice from the field “One of the most powerful experiences of my professional career was talking to a young woman-through a crack in the steel door of her cell-who had been in prison for five years and isolation for the past eighteen months. She was agitated, panicky, and scared as she was scheduled to be released the following week and had nowhere to go. She was someone who was almost certainly abused as a child; had some degree of mental illness; had not made a meal or done laundry in years;
- 60. had no high school degree; and had been alone for the last year and a half in a room smaller than my bathroom, and would soon be released without support or assistance. I couldn't imagine that she would not end up in some type of prison or mental health facility. Without extensive support and involvement from social workers both before and after release, which our current system does not allow, this young woman is almost certain to fail.“ (Brown, A., Social Worker and Prison Monitor in IL) The COVID-19 pandemic has revealed the best and the worst of us. As we continue to respond to the crisis in the US, there is increasing media coverage of the impact of the pandemic for justice-involved people. Please review media sources for articles that you can directly relate to earlier topics in this class such as racism, mental health problems, addiction issues, challenges of reentry, prison conditions, etc. In this post please summarize the article and link it to class topics. For a great collection of media articles dedicated to the criminal justice system, please see The Marshall Project website.