
Recommended
Recommended
More Related Content
More from vannagoforth
More from vannagoforth (20)
Recently uploaded
Recently uploaded (20)
Original Articles and ReviewsThe Psychology of Euthanasia.docx
- 1. Original Articles and Reviews The Psychology of Euthanasia Why There Are No Easy Answers Miguel Ricou1,2 and Tony Wainwright3 1Faculty of Medicine, University of Porto, Porto, Portugal 2Department of Psychology and Education, Portucalense University, Porto, Portugal 3Department of Psychology, University of Exeter, UK Abstract: Voluntary euthanasia has been legalized in several countries and associated with this development there has been much discussion concerning the relationship between the ethical principle of autonomy and the respect for human life. Psychological science should make a significant contribution to understanding how polarizing positions may be taken in such debates. However, little has been written concerning the implications of this research for the euthanasia debate and about the contributions of psychology. In the same way, very little is written about the psychologist’s role in countries where voluntary euthanasia or assisted suicide is legalized. We take as a starting assumption that there are no solutions that will meet everyone’s wishes or needs, but that an understanding of psychological ideas, can assist in developing strategies that may help people with opposing views come to some agreement. In our view, it is fundamental to a fruitful
- 2. analysis, to leave aside a polarized approach and to understand that an eventual answer to the question of how we approach voluntary euthanasia will only be achieved after the hard process of carefully considering the consequences of having either legalized voluntary euthanasia or its prohibition, in the context of a psychological understanding. Keywords: euthanasia, suffering, psychology, ethics, decision- making Voluntary euthanasia has been legalized in several coun- tries,1 and in others it is being considered. This trend toward legalization has led to much debate concerning competing ethical principles (Youngner & Arnold, 2016). As an example, in Portugal, where discussion about legisla- tion has been in progress for some time, the head of Portu- gal’s national nurses association alleged that euthanasia is already being carried out, despite it currently being illegal (https://www.bioedge.org/bioethics/nurse-ignites-debate- over-euthanasia-in-portugal/11783) and this provoked intense debate and criminal investigations into the medical staff concerned. There are clearly very strong feelings involved here, but our contention is that there is no right or wrong answer. In discussing the issues arising from ethics at the end of life, as in the case of voluntary euthanasia2 or assisted suicide, our contention is that taking an absolutist position – that there is a “right or wrong” answer – will not be helpful. We intend to outline the boundaries between the values or principles that are in contention and to develop some ideas about how these may be, at least partially, reconciled, using psy- chological ideas as our framework.
- 3. When we consider the decision to end our life, either in the case of suicide or voluntary euthanasia, we are facing a complex challenge that involves privileging one of at least two main principles: the principle of autonomy which may be seen as also promoting respect for human dignity; or the principle of respecting life, also related to the princi- ple of nonmaleficence (Beauchamp & Childress, 2001). It is also the case that if you take the view, as we do, that there are no absolute values or principles here, (see, e.g., (Engel- hardt, 1999) the main decision for any society, is to draw a conscious and considered boundary between these two cen- tral values. Of course, many people hold that there are absolute values or principles, as in the case of some faith communities, but our view is that these can only be used a guide, not a prescription in secular societies where many faiths, and those with no faith, have to live together. Here we explore the consequences of either undervalu- ing the principle of autonomy, for example, in a society where voluntary euthanasia as a personal choice does not exist, and the parallel consequences where the value of life may be thought to be diminished in society where voluntary euthanasia is available as part of public policy. 1 In Europe Euthanasia and Assisted Suicide are legalized in the Netherlands, Belgium, and Luxembourg. Also in Europe there are two more countries – Switzerland and Germany – with laws allowing Assisted Suicide. In the rest of the World just in Colombia Euthanasia and Assisted Suicide are legal. In Japan, although there is not a law, Euthanasia and Assisted Suicide are not illegal. Assisted Suicide is also legal in Canada and in five states of USA – Oregon, California, Colorado, Washington, and Montana.
- 4. 2 Where we use the term euthanasia alone, we mean by this voluntary euthanasia. � 2018 Hogrefe Publishing European Psychologist (2019), 24(3), 243–256 https://doi.org/10.1027/1016-9040/a000331 T hi s do cu m en t i s co py ri gh te d by th e A m
- 7. he p er so na l u se o f t he in di vi du al u se r a nd is n ot to b
- 8. e di ss em in at ed b ro ad ly . This paper will also aim to explore the role that psychol- ogy can play in helping an individual make the best deci- sion, given their circumstances. There are very few published studies about psychology and hastened death, which is unexpected, given the importance of this area for clinical practice. We believe psychology should play a major role whether in the discussion of legalizing or not euthanasia or assisted suicide, or in the work with people who ask to die. Furthermore we will develop some ideas on the role of the professional psychologist in this field. Finally we hope to outline what psychology can contribute to the development of public policy in this area. Conceptualization and Definitions
- 9. It will be useful to introduce our argument with some his- tory and some definitions. Euthanasia comes from two Greek words: eu, meaning good, and thanatos, meaning death. Contemplating this, we can say that, at least in its original meaning, euthanasia refers the promotion of dying as a good experience (as far as that is possible) and so would include the idea of voluntariness as well as active engagement, even when this involves the assistance of another person. From a historical point of view it is believed that Francis Bacon was the first to write about euthanasia in a medical context in 1605 where he says: “Nay further, I esteem it the office of a physician not only to restore health, but to mitigate pain and dolors; and not only when such mitigation may conduce to recovery, but when it may serve to make a fair and easy passage.” (Bacon, 1605/2000, p. 100) Over the years, attitudes to euthanasia have changed, and particularly in Europe and the United States there have been increasing numbers of jurisdictions making voluntary euthanasia legal or at least decriminalizing it (Youngner & Arnold, 2016). One reason for the change in attitudes to voluntary euthanasia has been the rapid advance in medical treat- ment that has allowed life to be sustained much longer, for example, through intensive care, than hitherto. This has meant that increasing numbers of patients survive only by being kept alive through artificial means and has pro- duced situations in which ethical concerns raise major chal- lenges (McDermid & Bagshaw, 2009). It has also been argued that this shift in opinion reflects an even longer trend that has seen science and technology offer meth-
- 10. ods for fixing the world’s problems and even death is now seen as a possible fixable problem. Euthanasia could then be viewed as consistent with this idea, that it provides a way of controlling, if not preventing, death (Harari, 2016). In the UK, there have been many debates and legal chal- lenges to the current prohibition, but these have not been successful (Bowcott, 2017). Over 20 years ago, the UK House of Lords Select Com- mittee on Medical Ethics, for example, made a clear dis- tinction between prolonging life unnecessarily and the voluntary refusal of treatment – orthothanasia – on the one hand, and euthanasia on the other, and this distinction has been maintained ever since: autonomy in refusing treatment being maintained, but autonomy for receiving a lethal drug, for example, being denied. “With respect to euthanasia, may I first indicate that in our deliberations we defined voluntary eutha- nasia, at the request of the individual concerned, as being a deliberate intervention undertaken with the intention of ending a life so as to relieve intract- able suffering; an act which must inevitably termi- nate life. We were unanimous in concluding that the right to refuse medical treatment is far removed from the right to request assistance in dying.” (House of Lords Selection Committee on Medical Ethics, 1994) Defining Our Terms: Voluntary Euthanasia, Nonvoluntary Euthanasia, and Involuntary Euthanasia There are some further distinctions that need to be made,
- 11. as they play an important role in debates and firstly we deal with “voluntary euthanasia,” “nonvoluntary euthanasia,” and “involuntary euthanasia.” Voluntary euthanasia is performed with the consent of the person. This is the term that we shall be using when we discuss legalization later in this paper, as its fundamen- tal purpose is to respect the wishes and autonomy of the person concerned. The second term is nonvoluntary euthanasia where the person is not able to give consent. As a consequence it is harder to argue that here autonomy is being respected. However, in situations where the person lacks capacity, for example, they are in a coma or a persistent vegetative state, if food and fluids are withdrawn or life support is turned off, the procedure can be described as nonvoluntary euthanasia. This term is also commonly applied to cases in which the person is a minor and may not be able to make their own judgment. Usually, in these cases, it is the family who ask for euthanasia, representing the person’s will. In the same way, previously expressed wishes, as in advance European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe Publishing 244 M. Ricou & T. Wainwright, The Psychology of Euthanasia T hi s do cu m
- 16. ly . healthcare directives, can be on the basis of a nonvoluntary euthanasia, if at the time the person lacks capacity. The third term – involuntary euthanasia – refers to the sit- uation where the person is killed against their expressed will or, at least, without their consent. A major example was the Nazi T4 or “Euthanasia Programme,” where many disabled people were put to death, and indeed the first gas chambers were used for killing people with a learning dis- ability (Lifton, 1986). In more recent times the term has been applied to cases of euthanasia where it is alleged that consent was not given, or the person was not correctly assessed, raising doubts about whether the persons con- cerned had really expressed a wish to die (Singer, 2003; Gillon, 1999). Our literature review suggests there is insuf- ficient research on the psychological issues here, and that a much fuller application of psychology in the debates on how any policy is implemented, would be beneficial in avoiding some of the risks of involuntary euthanasia taking place. In the same way, it is possible to argue that when a society accepts voluntary euthanasia, as time goes by, the practice becomes more and more acceptable, so people are not so strict with the criteria that are applied for some- one to receive euthanasia (Pelligrino, 1998). In that way, voluntary euthanasia slides to involuntary euthanasia. We will come to this issue when discussing the idea of a “slip- pery slope.” Active Euthanasia, Passive Euthanasia, Orthothanasia, Disthanasia, and
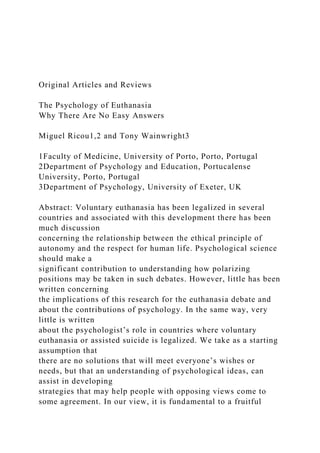
- 17. Physician-Assisted Suicide Finally there are some further terms that need to be made clear for the purposes of our discussion; these are active euthanasia, passive euthanasia, orthothanasia, disthanasia, and physician-assisted suicide (Table 1). In active euthanasia – a third person (usually a medical professional) deliberately does something that causes the person’s death – an act of commission. In passive euthana- sia something is not done – an act of omission – whereby the effect is the ending of the person’s life (an example of this might be a patient refusing medical treatment that would have kept them alive). The term orthothanasia (from the Greek “normal death”) refers to a person’s right to refuse treatment, even if this leads to their dying. The dif- ference in meaning between passive euthanasia and orthothanasia is that, in cases of passive euthanasia, people do want to die, while in cases of orthothanasia people do not want to die, per se, but rather want to deal with the neg- ative effects or consequences of their treatment or condi- tion. This difference makes it easier in general for people to accept the latter as ethically justified, and goes some way to explain why orthothanasia is usually legally accepted and passive euthanasia is not (Singer 1995). Another term that it will be useful to be clear about is dis- thanasia (from the Greek “bad death”). This refers to the situation, for example, where a person’s life is prolonged, perhaps against their will, through what may be regarded as disproportionate means, perhaps causing a person with an incurable condition additional and unnecessary suffer- ing. Disthanasia can be therefore understood in some ways as standing as the opposite of voluntary euthanasia as it may extend suffering instead of promoting its end by a
- 18. “good death.” Of course, disthanasia is an unacceptable practice in health care. The final term we would like to introduce is physician- assisted suicide. This describes the situation where a doctor provides a patient with the means to end their own life but Table 1. Definitions Person asks to die Person doesn’t ask to die because he/she is not autonomous Person doesn’t ask to die Person doesn’t want to die, but refuses treatment* Someone kills the patient
- 19. The patient kills themself with help Death resulting from withholding treatment Prolonging life with disproportionate means Active voluntary euthanasia X X Passive voluntary euthanasia X X Active nonvoluntary euthanasia X X Passive nonvoluntary euthanasia X X Active involuntary euthanasia X X Passive involuntary euthanasia X X Orthothanasia X X Dysthanasia X Physician-assisted suicide X X *Usually legal in most countries.
- 20. � 2018 Hogrefe Publishing European Psychologist (2019), 24(3), 243–256 M. Ricou & T. Wainwright, The Psychology of Euthanasia 245 T hi s do cu m en t i s co py ri gh te d by th e A m er
- 23. p er so na l u se o f t he in di vi du al u se r a nd is n ot to b e
- 24. di ss em in at ed b ro ad ly . takes no part in its administration – this being left to the patient themselves. Some have argued that from an ethical perspective, physician-assisted suicide and voluntary eutha- nasia are much the same (Brock 1995; Dixon 2012), since in situations where the administration of medication is the means of dying, whether it is administered by the doc- tor or by the patient, from an ethical perspective, makes lit- tle difference. Those who are in favor of physician-assisted suicide argue that in these circumstances, the patient is the ultimate cause of their own death, and this ensures that it really is their decision – that they were clearly motivated to take their own life. In the same way the possibility of sub- tle coercion, error, and other abuses are reduced (Battin 1991; Quill, Cassel, & Meier 1996). One issue that these definitions have in common con- cerns the motivation of the person concerned and raises
- 25. an important question of how can this be assessed. How sure can we be that the person is motivated to die for the “right” reasons and not being pressured into it by others, or by a mistaken belief that this is the only course open to them? Research on those who narrowly escape killing themselves in suicide attempts support the idea that people can change their minds and often do (Seiden, 1978); but for those who are successful, there is no way of knowing of course. Nevertheless, we can argue that those who defend assisted suicide, as a way to ensure that the person’s moti- vation is fully engaged with dying, is to admit that in gen- eral, it is hard to be sure what someone’s real reasons are when they are asking to die. We will come back to that when we will be discussing the role of psychology. Euthanasia – Potentially Conflicting Values Values and Social Norms The question of euthanasia and human rights, their rela- tionship with personal values, and how they may come into conflict with each other, is an important theme in this dis- course. In addition, social norms change as societies develop and the interplay between social norms and per- sonal values is an important further consideration. In gen- eral, societies across the world and their associated cultures have been evolving in a way that promotes human rights in many different ways and so the discussion of euthanasia is often located in that framework, that is, a dis- cussion about rights (Pegram, 2015). The first of these personal values is dignity and there has been an increasing focus on people’s dignity, and other
- 26. rights, that enlarge a person’s opportunity to differentiate themselves from others, and to assert their own individual identity (Pinker, 2011). In such a framework, each individ- ual is taught that they are unique, making them the only one who truly knows what is best for them. One of the con- sequences of this is that when we are faced with a situation where we are trying to judge what is best for another per- son, it means accepting and respecting the other person’s will and also their autonomy, and only by doing this will we be treating them with dignity (Ricou, Sá, & Nunes, 2017). Another fundamental value that is clearly important in this context is how we judge the importance or indeed the value of human life. It is a truism to say that people in general appreciate and value their lives, so it is almost impossible to imagine a modern society where human life is not respected. In fact, if people did not cherish life in their social relationships, the social order would swiftly break down. So in the context of this discussion of euthanasia, we are proposing that there are two central values that are in play: dignity (that is operationalized as respect for autonomy) and respect for human life. Absolute and Relative Values Whether values are regarded as absolutes or change depending on circumstances has a significant impact on ethical decision-making (Neumann & Olive, 2003). Taking the position that there are absolute values or principles is to accept that there are absolute right things and absolute wrong things, which is contrary to the global consensus that people have different world views. Of course, respecting differences does mean accepting that we live in a world where people with absolute values and people with more
- 27. relative values will need to coexist. In clinical practice, given this situation, professionals working with absolute principles will find particular ethical challenges, since they will need to work with everyone including those whose values differ from their own (Page, 2012). Beauchamp and Childress (2001), in their moral common theory, talk about middle-level principles. These are principles that can be considered absolutes, except when they conflict between each other. When they do con- flict, the professional should analyze the situation and define which principle should be, in that particular situa- tion, prioritized, and should try to reach some form of resolution. As argued later in this paper, in the case of euthanasia, there is a conflict between the principle of autonomy and the principle of nonmaleficence; neither one nor the other can be treated as an absolute, but they are extremely European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe Publishing 246 M. Ricou & T. Wainwright, The Psychology of Euthanasia T hi s do cu m en t i
- 30. le is in te nd ed s ol el y fo r t he p er so na l u se o f t he in di
- 32. important. Our main goal is to understand the possible implications of the overvaluing of one principle compared to the other. What can happen if we overvalue autonomy compared with nonmaleficence when accepting euthana- sia? On the other hand, if we overvalue nonmaleficence, are we being paternalistic? And how can we evaluate people to understand if what they are expressing represents his or her best interest? In conclusion, if we accept that there are no absolute principles, the role of the health professional is to choose, in each particular case, which principle should be priori- tized. Because the values we are talking about (value of autonomy and value of life) are strongly endorsed in con- temporary western societies, with differing views about how they should be implemented, it is not reasonable to leave these decisions alone to the health professional. The legal system is the vehicle through which such competing views can be regulated that provides the overall framework. The best law needs to take account of the possible conse- quences of the different possible choices and we explore that in the remainder of this paper. Respecting Autonomy A psychologist, in the same way as a medical doctor, always works intending the best outcome for his client or patient. The difficulty is to understand, in these cases, what repre- sents the best outcome, respecting life or respecting autonomy. It is known that well-being is highly related to the per- son’s ability to adapt to new circumstances in life. When
- 33. something, like a terminal disease, happens in a person life, suffering will prevail if the person is not able to adapt to the new circumstances imposed. Respecting autonomy is respecting the way the person thinks it will allow them to adapt and have the chance of pursuing a fulfilling future. In this way respecting someone’s autonomy is also a way to promote the person adaptation, because only the person knows the best way to adapt to the changes that have befal- len them. Nevertheless, whereas autonomy is an important guiding principle, it is insufficient to capture the full range of com- plex issues involved in end-of-life decision-making (APA, 2000). People change their minds often and there is sub- stantial variation in the will to live which suggests that a desire to die is inherently changeable (Maier & Newman, 1995; Chochinov, Tataryn, Clinch, & Dudgeon, 1999); there are emotional states that can interfere with people’s deci- sions; we know people can be rational but the decision pro- cess is not simple and involves many, sometimes competing, variables (Haidt, 2001; Damásio, 2010). The decision to commit suicide is a good example of the difficulty we face in understanding if a person’s decision always represents the best decision as we know from psy- chological science that decision-making under stressful cir- cumstances is subject to biases that may not lead to the best outcome (Mather & Lighthall, 2012). Given this evidence- base we believe that psychology has a major role to play here. Euthanasia and Suicide – A Right or an Absence of Choice Euthanasia, Suicide, and Rights Issues concerning euthanasia are closely connected with
- 34. those surrounding suicide. It is only in recent times that sui- cide has been decriminalized in some countries and it is still regarded as deeply wrong by many of the major world reli- gions and indeed, perhaps because of this, religious belief may act to reduce suicide risk (Cook, 2014; Lawrence, Oquendo, & Stanley, 2016; Stack & Kposowa, 2011; Wu, Wang, & Jia, 2015). So the question arises, should there be a legal right to suicide? In most jurisdictions where it is no longer a criminal offense, there is no right to suicide as such. If we were to advocate for such a right, how would we go about defining it? There would be strong views about this on both sides, as some people would regard suicide as acceptable as it would fit with their views about personal autonomy, whereas others would regard it as, for example, in the Catholic Church, as a Mortal Sin. We believe, no matter the perspective someone can have about suicide, that it would be possible for someone to want to die (Schramme, 2013). So, the question should be if we, as a society, should let people do it, or should we restrain them, because it would be always impossible to know, for sure, which people, between the ones who express the idea of committing suicide, want really to die and which people will change their minds. Different Types of Suicide One question that arises is whether there are different types of suicide and we can turn to Durkheim’s classic study (1897/2001) and list four types of suicide: egoistic, anomic, fatalist, and altruistic. Considering this last, it becomes obvious that suicide can have social motivations: the indi- vidual kills himself due to a social cause which he/she con- siders a more important value than his own life. In the case of a suicide bomber carrying out a terrorist attack, for instance, there is a belief in a more important value than the innate wish to preserve one's own life (Joiner, 2014).
- 35. Given this, we can say that suicide may be a rational option; a person may chose to die in a rational way. � 2018 Hogrefe Publishing European Psychologist (2019), 24(3), 243–256 M. Ricou & T. Wainwright, The Psychology of Euthanasia 247 T hi s do cu m en t i s co py ri gh te d by th e A
- 38. r t he p er so na l u se o f t he in di vi du al u se r a nd is n ot to
- 39. b e di ss em in at ed b ro ad ly . Sleek (1996) also states an important point regarding sui- cide: when it is performed by individuals who live with an incurable disease it can be seen as providing a sense of comfort once it gives the patient the chance to choose the moment he/she is going to die. In the opposite way, we also know that, often, people claim they want to die and after all they change their minds. How Do We Know if Someone Would Regret Their Decision if They Lived? One key fact here is that most of the people with suicidal intention, or even having attempted to kill themselves, end up changing their minds (Maser et al., 2002). Only a small minority go on to commit suicide (Klonsky, May, &
- 40. Saffer, 2016). However, of course, this data is compromised as we cannot ask those who do commit suicide whether they had a change of heart before they died. Nevertheless, given this discussion, it is always possible for a person to change their mind. They may wish to die at a particular moment, but if they survive, they may be very grateful. On the other hand, they may not, and telling the difference between these two situations is very difficult. From the evidence that we have, it is relatively common for people to have second thoughts, so that it is clearly better to err on the side of assuming that someone may change their minds as if they do die, there is no chance to regret it or otherwise. The Role of Professionals While there are no absolute methods for assessing a person wishes and whether they are likely to change their minds concerning their wish to die, psychologists always draw on whatever scientific evidence is available to inform their judgment; this means that their starting assumption is that it would be highly probable that the person might wish to die at one point in time but would be likely to change their minds. But this issue becomes more complicated for doctors. Usually they are the only professional group that would are legally accredited to perform euthanasia, where it is legal3 (Pereira, 2011). And why is that? Medical codes of ethics are clear; they must relieve a patient’s suffering and/or cure them whenever possible. Therefore, when con- fronted with a patient whose pain or disease cannot be cured and they are likely to continue suffering despite treat- ment, the doctor considering their obligation to relieve the suffering, can think about euthanasia being in the patient’s best interests.
- 41. Taking into account the question of euthanasia, doc- tors and psychologists roles are particularly different as the former ought to decide whether to inject a lethal dose of drugs in the patient and the latter works with the possi- bility of the person wanting to live and therefore explores that chance, not having to accept death nor the means of inducing it. But a bigger moral issue can be generated if we think about a great mistake: keeping alive a person who wants to die and letting a person die who wants to live. How do we act if it is not possible to know for sure if the person will change their mind or not? Perhaps it would be fair to agree that, after knowing the person very well, and understanding their particular situation, it would be possible to make an informed guess about whether the person will or will not change their mind concerning their wish to die.4 Neverthe- less to build a law without a scientific evidence-base to eval- uate these possibilities it would be a very hard task, if not impossible. In that way, psychology has the responsibility to develop knowledge that would be able to bring more light in this subject. The Need for a Law Due to the importance of respecting autonomy and also respecting life, given the risks of a mistake that would result from privileging either in any particular case, our view is that only legislation can provide the necessary safeguards. This is one of the great paradoxes professionals face since they should always make decisions in line with their profes- sional principles (Ricou et al., 2017). In each case they should always consider the particular circumstances for each person and what would be in their best interests. Rules, deontological and legal ones, are made for general or normal situations, and it is impossible to have a law that
- 42. will get the best solution for everyone (Vilches, 2001). Rules and laws represent the professional or social norm and are a clear guide, but each person is an individual and may or may not conform to these norms. Given that everyone is different and has differing needs, the responsibility of each professional is to decide, taking into account, but not being controlled by, these norms, adapting their practice to each person. That’s why professionals shouldn’t slavishly follow rules, they should work with their guiding ethical principles. Of course they need to know the rules, because they can’t disrespect them, but they have the responsibility to try solutions that will fit in the rules but solutions found after a professional reasoning based in the professional principles. 3 Switzerland seems to be the only exception to that. It is possible there, for nonmedical doctors to perform the assisted suicide. It only requires that the motive be unselfish (Hurst & Mauron, 2003). 4 It is clear in this statement the importance of a multidisciplinary work. To assess, counseling, understand the social and family context, know the patient’s problem or disease you need, at least, doctors, psychologists, nurses, and social workers. In fact, you need the same health professionals usually are part of a palliative care team. European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe Publishing 248 M. Ricou & T. Wainwright, The Psychology of Euthanasia T hi
- 47. ed b ro ad ly . Of course, rules are made, in part, because people in gen- eral can’t have the responsibility to decide simply using their own principles, at least about important societal val- ues. Euthanasia potentially puts into conflict two funda- mental values, so clearly society will need rules and laws. The consequence may be, of course, that it will be more dif- ficult to find solutions that will fit the best interest for each person, because the rules will cover general circumstances, not particular cases. In this way we need to find the fairest rules, including all the possible criteria to try to provide solutions in most situations, knowing that it will not be possible to find a solu- tion that fits everyone’s interests. This is the profes- sional role, trying to find and advocate for the best client solution; this is also where science can play a part, trying to develop the knowledge and evidence-base to make more fair laws, a research field that has not had the attention it deserves. Crisis, Pain, Suffering, and Decision-Making Crisis Having discussed the relationship between suicide and
- 48. euthanasia it is clear that both situations are associated with some sort of crisis in a person’s life. The term “crisis” has been defined as a decisive change, an acute moment of imbalance (Jalley, 2001), in other words, a turning point. The particular form of the crisis will vary but facing death inevitably leads to a reassessment of the person’s relationship with others, and indeed of their own life history. This can itself be a painful process and can be seen as both a cause and also an outcome of this critical transition – from life to death. However, life crises are not necessarily of such magnitude and while they may be challenging, they can be an important source of change and development. Indeed the research on post-trau- matic growth as a counter to overly pessimistic approaches to difficult experiences is a case in point (Chen & Wu, 2017). Suffering The concept of suffering is not straightforward, either in the context of either physical or psychological pain. Raus and Sterckx (2015), in their chapter on euthanasia and mental suffering, provide a comprehensive overview of the differ- ent ways in which this construct has been understood. Their particular focus was the rationale for allowing euthanasia for conditions where a diagnosable condition could be iden- tified and where there was severe suffering, but not where the same suffering was encountered without such a diagno- sis. Their conclusion is that the logic and ethical validity for this distinction is weak, but nevertheless there are grounds for maintaining it. How people respond to pain therefore takes many forms (Cassel, 1982). The literature has many definitions of psychological pain and there have been self- report measures associated with these definitions. These
- 49. have been shown to have some limited validity and reliabil- ity, although some are better than others (Tossani, 2013). As a summary, we can affirm that the role of suffering in a person’s life can play a positive role in personal develop- ment; in other words, suffering can lead the individual to mobilize their energy toward an adaptation to the circum- stances that led to the suffering, and to act on them. In this way, suffering can be transformative. However there will be situations where the challenge of adaptation is too great. Under these circumstances a person may request euthanasia, as they do not see any prospect of being able to adapt. It is probably impossible in principle to distinguish people who can adapt from those who cannot; though, it is clear that for some people under some circumstances adaptation would be highly improbable. Nevertheless, as mentioned earlier in this article, people do change their minds and a particularly clear example is known as the “Oregon Para- dox” (Lee, 2010). Here people, who go through the various complicated steps of being assessed for euthanasia and suc- cessfully receive the necessary clearance, experience a boost to their well-being and wish to live longer. The para- dox arises from the newly acquired capacity to end their lives sooner. While this has been seen in those with termi- nal illnesses, it may also apply to others where they achieve the option of ending their lives and this itself becomes a turning point. Decision-making about euthanasia is a difficult task and involves much emotional effort by the person involved, pos- sibly family and friends and the care team. This process is not easy and different people may have different capacities in this area (Dees et al., 2013).
- 50. This is the point where euthanasia could be considered – for those who cannot adapt – being clear, however, that it is very difficult to be sure about whether someone really can- not adapt, or just needs more time. Medical Doctors Conflicts With Beneficence and Nonmaleficence Having explored suffering, some aspect of which is associ- ated with a person’s request for euthanasia, and have briefly characterized issues concerning the right to life and personal autonomy, we shall now consider two related concepts from medical ethics: beneficence and � 2018 Hogrefe Publishing European Psychologist (2019), 24(3), 243–256 M. Ricou & T. Wainwright, The Psychology of Euthanasia 249 T hi s do cu m en t i s co py
- 53. te nd ed s ol el y fo r t he p er so na l u se o f t he in di vi du al
- 54. u se r a nd is n ot to b e di ss em in at ed b ro ad ly . nonmaleficence (Beauchamp & Childress, 2001), the injunction to only do good and never to do harm. Both of
- 55. these ideas are central to what you might call the “medical conscience” and will come into play when a request for euthanasia is made. Based on these considerations, we must take into account that all health professionals, such as doctors, are professionally obliged to pursue the well-being of their patients and avoid inflicting harm and it is clearly a chal- lenge to conceive of killing someone, even on their own request, as being consistent with this. This then leads to efforts to minimize suffering as much as possible, and to whether euthanasia would be one approach that would indeed minimize suffering (and through this reasoning legitimize it) or by contrast, bring the patients chance for future happiness to an end. Concluding this section there is a strong case to be made that there are some individuals under some circum- stances who would not be able to adapt to the situation and their life conditions are such that they may make a rational choice that death is preferable to life, hard though this is for a professional committed to saving life to accept. We can then draw the conclusion that respecting the per- son’s autonomy includes understanding that some people cannot adapt and would be condemned to suffer; and that for them, euthanasia would be a possible way to bring the suffering to an end. The problem, as already pointed out, is to accurately determine who those people are – some- thing we are currently unable to do. The Slippery Slope Argument – Respecting Nonmaleficence Having reviewed the main arguments that are made in sup-
- 56. port of the practice of euthanasia, we now turn to those arguments that are made to oppose it, and we will first con- sider the “slippery slope” (Pereira, 2011). This makes the case that once it is established, it becomes a socially accept- able norm, and is applied in ways that may never have been intended. A similar idea in military terms is called “mission creep” (http://tinyurl.com/euthanasia-mission-creep). The fear is that there is a gradual shift from voluntary euthanasia, with informed consent, and excellent safe- guards, to involuntary as the approach is more generally accepted, and the society is desensitized to the ethical con- cerns raised when euthanasia was first introduced. Essen- tially people get used to things. In addition, there are some strong arguments that the incentives will be there to extend the range of those who will be affected by this process. Incentives That Lead to “Mission Creep” Firstly, we shall consider the economic and financial ques- tion. In other words, keeping patients alive hooked into hos- pital machines becomes costly after a while and therefore, unplugging the devices, killing the patient, ends up being an economical benefit to the hospital as it stops the costs and frees up beds. (Finlay, Wheatley, & Izdebski, 2005) Since the global financial crash of 2008, there has been an emphasis on “austerity” policies that have had a major impact on health across Europe (Quaglio, Karapiperis, Van Woensel, Arnold, & McDaid, 2013) and it is not hard to imagine that with euthanasia a relatively cost-saving intervention, policymakers would become more interested in it. Pelligrino (1998, p. 87), an authority on palliative care medicine, made this point, when he wrote:
- 57. “In a society as obsessed with the costs of health care and the principle of utility, the dangers of the slippery slope. . .are far from fantasy. . . Assisted suicide is a half-way house, a stop on the way to other forms of direct euthanasia, for example, for incompetent patients by advance directive or sui- cide in the elderly. So, too, is voluntary euthanasia a half-way house to involuntary and nonvoluntary euthanasia. If terminating life is a benefit, the reason- ing goes, why should euthanasia be limited only to those who can give consent? Why need we ask for consent?” He also stresses that the healthcare managers and doctors have an interest in freeing up beds, so they can treat more patients, have better clinical outcomes for those that do not have euthanasia, and also for increasing profits. As we noted earlier, proponents of euthanasia argue that the main reason some doctors support voluntary eutha- nasia is because they strongly value the patients’ right to be treated as autonomous human beings who can make deci- sions involving what happens with their lives. Nevertheless, there is some evidence that cost-conscious doctors are more likely to honor their patients’ requests for death as a study carried out in 1998 found that those who are cost-conscious and “practice resource-conserving medi- cine” are significantly more likely to write a lethal prescrip- tion for terminally-ill patients (Sulmasy, Ely, & Sprung, 2016; Sulmasy, Linas, Gold, & Schulman, 1998). Putting this into a broader context, we know from the field of behavioral and organizational ethics that perverse incen- tives like this play an important role in calibrating ethical decision-making (Bazerman & Banaji, 2004; Bazerman & Tenbrunsel, 2011).
- 58. The issue of cost saving can work both ways, however. It is possible that the money saved by offering the choice of European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe Publishing 250 M. Ricou & T. Wainwright, The Psychology of Euthanasia T hi s do cu m en t i s co py ri gh te d by th e
- 61. fo r t he p er so na l u se o f t he in di vi du al u se r a nd is n ot
- 62. to b e di ss em in at ed b ro ad ly . euthanasia would release funds for improving palliative care and other hospice services. It may also work, in the opposite direction, where there would be an argument that palliative care would become increasingly unnecessary as people would be encouraged to take up the offer of eutha- nasia rather than extending their lives with more complex treatments. As noted by Pelligrino (1998), another concern is if vol- untary euthanasia were to become legal, it would not be long before involuntary euthanasia would occur. A person might feel pressure, whether real or imagined, to request euthanasia in order to relieve the family’s suffering or dis-
- 63. tress caused by the person’s illness or its costs, especially where the family has few resources. One of the main rea- sons people give for asking to die is feeling a burden to their families (Kelly et al., 2003; Lulé et al., 2014). It is also pos- sible that the family may encourage the person to request euthanasia, in either direct or more subtle ways. In these situations the person concerned is quite vulnerable and it is not difficult to imagine that they might feel pressurized to seek an early death. Under these circumstances, it would be important to assess the wider context. If they were under such pressure, can we really call it a voluntary decision? Putting aside considerations of direct family pressure, where euthanasia has become established and is seen as a normal option, people may feel a more general social pressure to end their life, as they will be seen, and may see themselves, as taking resources away from others who may be thought to be more entitled.5 Finlay et al. (2005) also point out that once patients have the choice of euthanasia, doctors will feel under an obliga- tion to offer it for all those who are eligible, even to those who have not asked about it. There is then a consequential risk of lowering the patients morale and lead them to take an option they would prefer not to take. So here we see some of the limitations on our ability to judge autonomous decision-making and leads logically to questioning how legitimate it is to regard the person as fully autonomous. This is particularly problematic and raises fundamental issues of responsibility since, of course, eutha- nasia once administered is not reversible. The question of whether there is a slippery slope is now an empirical one. There are jurisdictions where euthanasia has been an option for many years, and it is possible to see
- 64. how far the changes predicted with this argument have happened. There is a mixed story here and arguments on both sides, although the consensus is that there are exten- sions to the original law likely to take place. This can be seen, for example, in the Belgian experience where the choice is now extended to children, where this would not have been considered when the initial laws were passed (Byock, 2016). The Role of Psychology As we have discussed, one of the major problems in decid- ing whether euthanasia can be in the person’s best interest, is related to limitations in our ability to judge autonomous decision-making. In situations where the national law per- mits euthanasia or assisted suicide, we believe psycholo- gists skills set can play a role in evaluating a client’s ability to make an informed decision; we also believe their knowledge and skills can also evaluate the degree to which the wish to die is likely to persist over time. In every case, psychologists should have a continuing role as part of their counseling relationship. However, this is not apparently happening both in countries where hastened death is legal or illegal (see below). The Role of Psychology: Literature Review In the literature review we conducted concerning psychol- ogy and hastened death, we found very little evidence about the role of psychology or of psychological practice. The research was carried out in the electronic databases APA PsycNET, EBSCO, EuropePMC, PubMed, Sage, Scien- ceDirect, SpringerLink, Wiley Online Library. We also used the Google search engine. The keywords euthanasia,
- 65. assisted suicide, hasten death, desire to death, end of life decisions, and psychology were used in English and Por- tuguese. The combination of words used was euthanasia and psychology; assisted suicide and psychology; hasten death and psychology; desire to death and psychology; and end of life decisions and psychology. To guide the selection of the articles, inclusion, and exclusion criteria were defined. Inclusion criteria were: (a) the publications between 2000 and 2017; (b) texts in English and Portuguese; (c) studies in the field of psychology and/or that consider psychosocial factors; and (d) quantitative and qualitative surveys were considered. As it is a theme that was not well represented in the litera- ture, we also included literature reviews or theoretical dis- cussion about euthanasia and psychology and/or assisted suicide and psychology. Exclusion criteria included: (a) studies in other languages; 5 It is curious to know that in the Netherlands the feeling that one is a burden to others can be a factor contributing to the unbearable nature of suffering, so a criteria to accept voluntary euthanasia (Regional Euthanasia Review Committees [RTEs], 2016). � 2018 Hogrefe Publishing European Psychologist (2019), 24(3), 243–256 M. Ricou & T. Wainwright, The Psychology of Euthanasia 251 T hi
- 70. ed b ro ad ly . (b) studies that did not consider themes in the field of psy- chology; and (c) studies preceding year 2000. Applying the inclusion criteria we just identified 17 articles. Most of them (9) are from Canada (Galbraith & Dobson, 2000; Rodin et al., 2008; Wilson et al., 2000, 2007) and Australia (Hudson et al., 2006; Kelly et al., 2003; Mitchell & Owens, 2000; Robinson, Kissane, Brooker, & Burney, 2017; Sanson et al., 2008), 2 from United States of America (Emanuel, Fairclough, & Emanuel, 2000; Suarez-Almazor, Newman, Hanson, & Bruera, 2002) and just 6 are from Europe (Bellido-Pérez, Monforte-Royo, Tomás-Sábado, Porta-Sales, & Balaguer, 2017; Caputo, 2015; Lulé et al., 2014; Mystakidou, Parpa, & Katsouda, 2005; Mystakidou, Parpa, Katsouda, Galanos, & Vlahos, 2004; Rodríguez-Prat, Balaguer, Booth, & Monforte-Royo, 2017) and none of them from countries where hasten death is legalized. Seven are literature reviews or theoretical discussion. In three papers (Galbraith & Dobson, 2000; Mitchell & Owens, 2000; San- son et al., 2008) the authors argue that psychologists should be involved in the capacity assessment process, which we believe is logical. Nevertheless, we believe psy- chology should go further and try to assess not just capacity
- 71. but also the ability to make really informed decisions. Sev- eral studies about suicide (Maia & Ricou, in press) show that there are some factors that contribute to the probability of people committing suicide. It would be important to understand which of those factors can contribute to hasten death request. All the others articles just mention the gen- eral role of psychologists, as in counseling and alleviating distress with families. In the same way Sanson et al. (2008) advocate that psychologists should play a role in decisions, advocacy and with the work after euthanasia with families and professionals. Nevertheless, none of those papers suggest any kind of intervention techniques. There is an inventory for assessing the wish to hasten death, appar- ently the most widely used (Bellido-Pérez et al., 2017). In one systematic literature review (Caputo, 2015) the main conclusions were very similar; that there is a little role for psychology in situations where there has been a request to hasten death. Ten articles studied patients’ perceptions about the legal- ization/acceptance of euthanasia or assisted suicide in terms of psychological and social factors. The wish to die was frequently associated with less religiosity, reduced functional status, pain, lower levels of social support, and loss of dignity. Most of the papers indicate that greater per- ception of being a burden for others and a diagnosis of depression were the main factors contributing for the wish to die. Depressive symptoms are naturally very common in those patients and consequently the diagnosis is difficult to make. None of those papers discuss the level of depression that should be considered as grounds for accepting or rejecting the wish to die as valid. Nevertheless two papers (Emanuel et al., 2000; Wilson et al., 2007) argue that depression can increase the probability of the patient changing their minds about hastening death, so they pro-
- 72. pose psychologists have an intervention role with those patients. Feeling a burden to others is one of the other most cited reasons for the wish to die. The main motivation, in this case, is the patient’s perception that they are the cause of suffering for other people, not their own suffering. Feel- ing a burden it is one of the reasons for suffering considered grounds for a euthanasia request in the Netherlands’ law. It is stated that the feeling that one is a burden to others can be a factor to contribute to the unbearable nature of suffer- ing (RTEs, 2015). Nevertheless it would be important to understand, in those cases, if the family actually feel the patient as a burden, and what kind of suffering the patient’s decision to die will cause in that same family. This should be, probably, another task for psychologists. Someone considering choosing to die is facing perhaps the most important decision a person can take, one laden with very significant psychological issues. Given both the significance to the person and these important psychologi- cal dimensions, psychological professionals need to become much more visible in end of life decisions (APA, 2000) and play a much more central role on the ongoing debate (Caputo, 2015). Psychologists have several areas of compe- tence, including assessment, counseling, and research that can contribute to the support of dying persons and/or to persons who express a wish to die. These skills include identifying factors that can be defined as catalysts or as inhibitors of the client ability to adapt perhaps personality or other individual factors. There is not a strong evi- dence-base supporting the work of psychologists in this field, but psychological studies in the associated field of sui- cide prevention shows that it would be possible to under- stand much more about these wish to die requests (Maia & Ricou, in press). Another issue is clarifying how likely is it that the
- 73. client will either change their mind, and adapt to the cur- rent situation, or remain convinced that death is the best option; and how long should be allowed for this process. As we have already stated (Emanuel et al., 2000; Wilson et al., 2007), there are correlations with depressive symp- toms, there being a higher probability of changing their mind about wish to die, the higher their depression score. But which other variables can contribute to it? And, how long should we wait for the person to change their mind? And what can the psychologist do in the meanwhile working with the patient? All those questions need answers that can have a strong influence in a law about euthanasia European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe Publishing 252 M. Ricou & T. Wainwright, The Psychology of Euthanasia T hi s do cu m en t i s co py ri
- 76. nd ed s ol el y fo r t he p er so na l u se o f t he in di vi du al u
- 77. se r a nd is n ot to b e di ss em in at ed b ro ad ly . or assisted suicide and currently the evidence is not available. The psychologist needs to also be mindful of the external
- 78. factors that may come into conflict with the person’s deci- sion. Sanson et al. (2008) propose an advocacy process with the patient and his/her family to better understand the motivations for dying. We also believe this should be a task for psychologists more than any other professionals given their specific skills set and knowledge base. Identifying individuals where there is absolutely no doubt about their wish to die, and who would maintain this wish and would benefit from the opportunity to do so is an impossibility. Society, through the law, has to provide a timeframe where it will be acceptable to reach a credible decision, and psychology can provide what research evi- dence there is to support the development of such a time- frame. In another way psychologists could play an important role in public and other professional’s education about issues related to death (APA, 2000; APS, 2008; San- son et al., 2008). As noted above psychologists can have a powerful influ- ence on clients’ decisions. Because of this, psychologists should always recognize the possibility for biases in their work, particularly being aware of their own views about euthanasia and assisted suicide. They should be highly cog- nizant about their personal opinions concerning euthanasia so they can work in an appropriate way (APS, 2008). They also should have proper training in the field of end-of-life psychology to ensure they have the skills and competence in assessing and counseling with this client group. Psychologists also play an important role working with the families of clients who ask to die. Sometimes, there can be conflicts between family members, and perhaps between family members and the client about the best way forward. Psychologists can play a role facilitating com- munication, and helping families to resolve or reconcile
- 79. such issues. In the same way psychologists can help other health professionals involved in such challenging situations and also support them in dealing with the powerful emo- tions that can arise. There is much research about suicide and palliative care, but very little about end-of-life decisions (Carmona, Santos, & Fonseca, 2011; Caputo, 2015). This is an area where psychological science should develop its research effort so that we improve our ability to assess how final the wish to die is in these situations and also about the way this kind of wish, where there are irrevocable conse- quences develops. Psychology can contribute to the design of a legal framework that takes account of personal vari- ables that contribute to the wish to die being a finalized choice, thereby avoiding as far as possible, non-intentional involuntary euthanasia. Final Considerations Our conclusion from this review is that there is no panacea, meaning that the case of euthanasia has the form of a clas- sical ethical dilemma, where there are problems with all the available options. When a society legislates on this subject – and there is no doubt at all that the conditions surrounding the process of dying ought to be legislated – the law is likely to be framed as one that is considered most suitable to most people in most cases. By definition, that idea sepa- rates us from casuistry, which shall be considered by the health professionals, but escapes from legal and legislative control. Given this possible legal framework for euthanasia, it fol- lows that, despite the approach taken having widespread social support, it will always be unfair to some people, as is the case with any legislation. Given this, it again follows
- 80. that in a society where euthanasia is an active practice, there will be people who even though they meet the criteria previously established for euthanasia, and also consciously affirm their wish to die, would not, in fact, actually want it. As discussed earlier, we know people who very clearly say they want to die, and even attempt to kill themselves, but change their minds. In these cases, there is a risk that those people would die even though they had the capacity to adapt to their situation and therefore to end their suffer- ing in other ways. For those who die, of course, this could never be determined as this process – euthanasia – is irre- versible, and this should be a reason to be more sure when considering someone request for dying than for any other reason. Likewise, we also must not disregard the fact that in soci- eties where euthanasia is legally forbidden, there will be people incapable to adapt to their situation, unable to relieve their suffering and hence will genuinely want to die and will not be allowed to, being condemned to live with their suffering. The main problem will always be to determine who in fact are those people that we can state without a single doubt that they truly want to die; knowing that, legalizing euthanasia, the tendency will be a slippery slope; summariz- ing, we have to be conscious that we face a major dilemma which consists in both situations: of keeping alive a person who wants to die and letting die a person who wants to live. In conclusion, whatever the choices defined by any soci- ety are, it will be fundamental to acknowledge the lack of perfect solutions to this matter which would solve every- one’s situations. Thus, it is essential to take into account the possible and predictable consequences of adopting
- 81. one or other policy, in order to reduce to the minimum the injustice that any decision at this level will cause to some people. The decision will always be the one � 2018 Hogrefe Publishing European Psychologist (2019), 24(3), 243–256 M. Ricou & T. Wainwright, The Psychology of Euthanasia 253 T hi s do cu m en t i s co py ri gh te d by th e
- 84. fo r t he p er so na l u se o f t he in di vi du al u se r a nd is n ot
- 85. to b e di ss em in at ed b ro ad ly . considered less onerous to the majority, but should put greater emphasis on protecting all of those who can become more vulnerable according to the choices made. Psychology has, in this context, a major role to play. Nevertheless, as far as we have been able to ascertain, psychological profes- sionals are not specifically included in any legislation con- cerning euthanasia or assisted suicide. Furthermore there are very few studies in this important area. Most of the pub- lications concern the issues arising from conflicting princi- ples and very few about decision-making in the context of dying. When someone is aware of all the possible problems
- 86. and/or merits of legalizing or not euthanasia, they will be able to find the best solution. Democracy works after the choices of people, where the majority take the lead role. So, in the ideal situation is for there to be very widespread understanding of these issues and the decision should be taken by the majority, or we believe better still, by those elected to represent the people. We have then a long path to walk, to develop knowledge that helps us to better understand the way people choose and the way those choices represent in fact their best inter- est. Knowing this it would be possible to provide much more information for the general population about the pos- sible consequences of maintaining or changing the law. References American Psychological Association (APA). (2000). The APA work- ing group on Assisted suicide and end-of-life decisions. Report to the Board of Directors of the the American Psychological Association. Retrieved from http://www.apa.org/pubs/info/ reports/aseol.aspx Australian Psychological Society (APS). (2008). Psychological perspectives on euthanasia and the terminally ill. An APS discussion paper prepared by a working group of the Directorate of social issues. Melbourne, Australia: Australian Psychological Society Ltd. Bacon, F. (2000). The Oxford Francis Bacon IV (ed. Michael Kiernan) (From the original: The Advancement of Learning, 1605). New York, NY: Oxford University Press. Battin, M. (1991). Euthanasia: The way we do it, the way they do it.
- 87. Journal of Pain and Symptom Management, 5, 298–305. https://doi.org/10.1016/0885-3924(91)90053-7 Bazerman, M., & Banaji, M. (2004). The social psychology of ordinary ethical failures. Social Justice Research, 17, 111–115. https://doi.org/10.1023/B:SORE.0000027544.56030.04 Bazerman, M., & Tenbrunsel, A. (2011). Ethical breakdowns. Harvard Business Review, 89, 58–65, 137. Beauchamp, T. L., & Childress, J. F. (2001). Principles of biomed- ical ethics (5th ed.). New York, NY: Oxford University Press. Bellido-Pérez, M., Monforte-Royo, C., Tomás-Sábado, J., Porta- Sales, J., & Balaguer, A. (2017). Assessment of the wish to hasten death in patients with advanced disease: A systematic review of measurement instruments. Palliative Medicine, 31(6), 510–525. https://doi.org/10.1177/0269216316669867 Bowcott, O. (2017, March 30). High court rejects challenge to ban on assisted dying. Guardian. Retrieved from https://www. theguardian.com/society/2017/mar/30/high-court-rejects- challenge-to-ban-on-assisted-dying Brock, D. W. (1995). Death and dying: Euthanasia and sustaining life. Ethical issues. In W. T. Reich (Ed.), Encyclopedia of bioethics (revised ed., pp. 563–572) Georgetown University. New York, NY: Macmillan Library Reference. Byock, I. (2016). The case against physician-assisted suicide and euthanasia. In S. J. Youngner & R. M. Arnold (Eds.), The
- 88. Oxford handbook of ethics at the end of life. Oxford, UK: Oxford University Press. Caputo, A. (2015). Trends of psychology-related research on euthanasia: A qualitative software-based thematic analysis of journal abstracts. Psychology, Health & Medicine, 20(7), 858– 869. https://doi.org/10.1080/13548506.2014.993405 Carmona, D., Santos, F., & Fonseca, S. (2011). Bioética, Eutanásia e Psicologia: Tecendo algumas reflexões [Bioethics, Euthanasia and Psychology: Making some reflections]. Mnemosine, 7, 188–203. Cassel, E. J. (1982). The nature of suffering and the goals of medicine. New England Journal of Medicine, 306, 639–645. https://doi.org/10.1056/NEJM198203183061104 Chen, J. L., & Wu, X. C. (2017). Post-traumatic stress symptoms and post-traumatic growth among children and adolescents following an earthquake: A latent profile analysis. Child and Adolescent Mental Health, 2, 23–29. https://doi.org/ 10.1111/camh.12175 Chochinov, H. M., Tataryn, D., Clinch, J. J., & Dudgeon, D. (1999). Will to live in the terminally ill. Lancet, 354, 816–819. Cook, C. C. H. (2014). Suicide and religion. The British Journal of Psychiatry, 204, 254–255. https://doi.org/10.1192/bjp. bp.113.136069 Damásio, A. (2010). Self comes to mind. Constructing the
- 89. conscious brain. New York, NY: Pantheon Books. Dees, M. K., Vernooij-Dassen, M. J., Dekkers, W. J., Elwyn, G., Vissers, K. C., & van Weel, C. (2013). Perspectives of decision- making in requests for euthanasia: A qualitative research among patients, relatives and treating physicians in the Netherlands. Palliative Medicine, 27, 27–37. https://doi.org/ 10.1177/0269216312463259 Dixon, N. (2012). On the difference between physician-assisted suicide and active euthanasia. Hastings Center Report, 28(5), 25–30. https://doi.org/10.2307/3528229 Durkheim, E. (2001). O suicídio. Estudo sociológico (7th ed.) (From the original: Le Suicide, 1897). Lisbon, Portugal: Editorial Presença. Emanuel, J., Fairclough, D., & Emanuel, L. (2000). Attitudes and desires related to euthanasia and physician-assisted suicide among terminally ill patients and their caregivers. JAMA: Journal of the American Medical Association, 284(19), 2460– 2468. https://doi.org/10.1001/jama.284.19.2460 Engelhardt, H. T. (1999). The foundations of bioethics. New York, NY: Oxford University Press. Finlay, I. G., Wheatley, V. J., & Izdebski, C. (2005). The House of Lords Select Committee on the Assisted Dying for the Termi- nally Ill Bill: Implications for specialist palliative care. Palliative Medicine, 19, 444–453. https://doi.org/10.1191/ 0269216305pm1062oa
- 90. Galbraith, K. M., & Dobson, K. S. (2000). The role of the psychol- ogist in determining competence for assisted suicide/eutha- nasia in the terminally ill. Canadian Psychology/Psychologie canadienne, 41(3), 174–183. https://doi.org/10.1037/h0086867 Gillon, R. (1999). Euthanasia in Netherlands–down the slippery slope? Journal of Medical Ethics, 25(1), 3–4. https://doi.org/ 10.1136/jme.25.1.3 Haidt, J. (2001). The emotional dog and its rational tail: A social intuitionist approach to moral judgment. Psychological Review, 108, 814–834. htps://doi.org/10.1037/0033-295X.108.4.814 European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe Publishing 254 M. Ricou & T. Wainwright, The Psychology of Euthanasia T hi s do cu m en t i s co
- 93. in te nd ed s ol el y fo r t he p er so na l u se o f t he in di vi du
- 94. al u se r a nd is n ot to b e di ss em in at ed b ro ad ly . Harari, Y. N. (2016). Sapiens: A brief history of humankind.
- 95. House of Lords Selection Committee on Medical Ethics. (1994). HL Deb 09 May 1994, 554, 1344–1412. Retrieved from http:// hansard.millbanksystems.com/lords/1994/may/09/medical- ethics-select-committee-report Hudson, P., Kristjanson, L., Ashby, M., Kelly, B., Schofield, P., Hudson, R., . . . Street, A. (2006). Desire for hastened death in patients with advanced disease and the evidence base of clinical guidelines: A systematic review. Palliative Medicine, 20(7), 693–701. https://doi.org/10.1177/0269216306071799 Hurst, S., & Mauron, A. (2003). Assisted suicide and euthanasia in Switzerland: Allowing a role for non-physicians. British Medical Journal, 326, 271–273. https://doi.org/10.1136/bmj.326. 7383.271 Jalley, E. (2001). La psychologie, une science fondée sur l'éthique? [Psychology - a science founded on ethics?] Le Journal des psychologues: Le mensuel des professionnels, 188, 8–9. https:// doi.org/10.3917/ess.021.0195 Joiner, T. E. (2014). The perversion of virtue: Understanding murder-suicide. Oxford, UK: Oxford University Press. Kelly, B., Burnett, P., Pelusi, D., Badger, S., Varghese, F., & Robertson, M. (2003). Factors associated with the wish to hasten death: A study of patients with terminal illness. Psychological Medicine, 33(1), 75–81. https://doi.org/10.1017/ S0033291702006827 Klonsky, E. D., May, A. M., & Saffer, B. Y. (2016). Suicide, suicide
- 96. attempts, and suicidal ideation. Annual Review of Clinical Psychology, 12, 307–330. https://doi.org/10.1146/annurev- clinpsy-021815-093204 Lawrence, R. E., Oquendo, M. A., & Stanley, B. (2016). Religion and suicide risk: A systematic review. Archives of Suicide Research, 20, 1–21. https://doi.org/10.1080/13811118.2015. 1004494 Lee, L. W. (2010). The Oregon paradox. The Journal of Socio- Economics,. https://doi.org/10.1016/j.socec.2009.10.008 Lifton, R. J. (1986). The Nazi Doctors: Medical killing and the psychology of genocide. Basingstoke, UK: Macmillan. Lulé, D., Nonnenmacher, S., Sorg, S., Heimrath, J., Hautzinger, M., Meyer, T., Kübler, A., Birbaumer, N., & Ludolph, A. (2014). Live and let die: Existential decision processes in a fatal disease. Journal of Neurology, 261(3), 518–525. https://doi.org/10.1007/ s00415-013-7229-z Maia, I., & Ricou, M. (in press). Can we ever accept a wish to die? Suicide and its link to euthanasia. Archives of Suicide Research. Maier, D. M., & Newman, M. J. (1995). Legal and psychological considerations in the development of a euthanasia statute for adults in the United States. Behavioral Sciences and the Law, 13, 3–25. https://doi.org/10.1215/03616878-29-6-1109 Maser, J. D., Akiskal, H. S., Schettler, P., Scheftner, W.,
- 97. Mueller, T., Endicott, J., . . . Clayton, P. (2002). Can temperament identify affectively ill patients who engage in lethal or near-lethal suicidal behavior? A 14-year prospective study. Suicide & Life- Threatening Behavior, 32, 10–32. https://doi.org/10.1521/ suli.32.1.10.22183 Mather, M., & Lighthall, N. R. (2012). Risk and reward are processed differently in decisions made under stress. Current Directions in Psychological Science, 21, 36–41. https://doi.org/ 10.1177/0963721411429452 McDermid, R. C., & Bagshaw, S. M. (2009). Prolonging life and delaying death: The role of physicians in the context of limited intensive care resources. Philosophy, Ethics, Humanities in Medicine, 4, 3. https://doi.org/10.1186/1747-5341-4-3 Mitchell, K., & Owens, R. (2000). Euthanasia and palliative psychology in end-of-life care. Australian Psychologist, 35(3), 193–200. https://doi.org/10.1080/00050060008257478 Mystakidou, K., Parpa, E., & Katsouda, E. (2005). The role of physical and psychological symptoms in desire for death: A study of terminally ill cancer patients. Psycho-Oncology, 15(4), 355–360. https://doi.org/10.1002/pon.972 Mystakidou, K., Parpa, E., Katsouda, E., Galanos, A., & Vlahos, L. (2004). Influence of pain and quality of life on desire for hastened death in patients with advanced cancer. International Journal of Palliative Nursing, 10(10), 476–483. https://doi.org/ 10.12968/ijpn.2004.10.10.16211 Neumann, J. K., & Olive, K. E. (2003). Absolute versus relative values: Effects on family practitioners and psychiatrists. Southern Medical Journal, 96, 452–457. https://doi.org/
- 98. 10.1097/01.Smj.0000054607.44960.49 Page, K. (2012). The four principles: Can they be measured and do they predict ethical decision making? BMC Medical Ethics, 13, 10. https://doi.org/10.1186/1472-6939-13-10 Pegram, T. (2015). Governing relationships: The new architecture in global human rights governance. Millennium-Journal of International Studies, 43, 618–639. https://doi.org/10.1177/ 0305829814562016 Pelligrino, E. D. (1998). The false promise of beneficent killing. In L. L. Emanuel (Ed.), Regulating how we die: The ethical, medical, and legal issues surrounding physician-assisted suicide (pp. 71– 91). Cambridge, MA: Harvard University Press. Pereira, J. (2011). Legalizing euthanasia or assisted suicide: The illusion of safeguards and controls. Current Oncology, 18(2), e38–e45. https://doi.org/10.1016/S0140-6736(03) 14520-5 Pinker, S. (2011). The better angels of our nature: Why violence has declined. New York, NY: Viking. Quaglio, G., Karapiperis, T., Van Woensel, L., Arnold, E., & McDaid, D. (2013). Austerity and health in Europe. Health Policy, 113, 13–19. https://doi.org/10.1016/j.healthpol.2013.09.005 Quill, T., Cassel, K., & Meier, D. (1996). Care of the hopelessly ill:
- 99. Proposed clinical criteria for physician-assisted suicide. Biomedical Ethics, 327, 1381–1383. https://doi.org/10.1056/ NEJM199211053271911 Raus, K., & Sterckx, S. (2015). Euthanasia and mental suffering. In M. Cholbi & J. Varelius (Eds.), New directions in the ethics of assisted suicide and euthanasia (pp. 79–96). New York, NY: Springer. Regional Euthanasia Review Committees [RTEs]. (2016). Annual Report 2015. Retrieved from http://www.euthanasiecommissie. nl Ricou, M., Sá, E., & Nunes, R. (2017). The ethical principles of the Portuguese psychologists: A universal dimension. Journal of Medicine and Philosophy, 2, 199–213. https://doi.org/10.1093/ jmp/jhw066 Robinson, S., Kissane, D., Brooker, J., & Burney, S. (2017). The relationship between poor quality of life and desire to hasten death: A multiple mediation model examining the contributions of depression, demoralization, loss of control, and low self-worth. Journal of Pain and Symptom Management, 53(2), 243–249. https://doi.org/10.1016/j.jpainsymman.2016. 08.013 Rodin, G., Christopher, L., Mikulincer, M., Donner, A., Gagliese, L., & Zimmermann, C. (2008). Pathways to distress: The multiple determinants of depression, hopelessness, and the desire for hastened death in metastatic cancer patients. Social Science & Medicine, 68(3), 562–569. https://doi.org/10.1016/j.socscimed. 2008.10.037
- 100. Rodríguez-Prat, A., Balaguer, A., Booth, A., & Monforte-Royo, C. (2017). Understanding patients’ experiences of the wish to hasten death: An updated and expanded systematic review and meta-ethnography. BMJ Open, 7. https://doi.org/10.1136/ bmjopen-2017-016659 � 2018 Hogrefe Publishing European Psychologist (2019), 24(3), 243–256 M. Ricou & T. Wainwright, The Psychology of Euthanasia 255 T hi s do cu m en t i s co py ri gh te d by
- 103. el y fo r t he p er so na l u se o f t he in di vi du al u se r a nd is
- 104. n ot to b e di ss em in at ed b ro ad ly . Sanson, A., Dickens, E., Melita, B., Nixon, M., Rowe, J., Tudor, A., & Tyrrell, M. (2008). Psychological perspectives on euthanasia and the terminally ill: An Australian Psychological Society discussion paper. Retrieved from https://www.psychology.org.au/Assets/ Files/euthanasia_position_paper.pdf
- 105. Schramme, T. (2013). Rational suicide, assisted suicide, and indirect legal paternalism. International Journal of Law and Psychiatry, 36(5–6), 477–484. https://doi.org/10.1016/j. ijlp.2013.06.008 Seiden, R. H. (1978). Where are they now? A follow-up study of suicide attempters from the golden gate bridge. Suicide & Life- Threatening Behavior, 8, 203–216. https://doi.org/10.1111/ j.1943-278X.1978.tb00587.x Singer, P. (1995). Rethinking life and death. New York, NY: St Martin’s Press. Singer, P. (2003). Voluntary euthanasia: A utilitarian perspective. Bioethics, 17(5–6), 526–541. https://doi.org/10.1111/1467- 8519.00366 Sleek, S. (1996). Ethical dilemmas arise treating AIDS patients. APA Monitor on Psychology, 27(6), 30. Stack, S., & Kposowa, A. J. (2011). Religion and suicide accept- ability: A cross-national analysis. Journal for the Scientific Study of Religion, 50, 289–306. https://doi.org/10.1111/j.1468- 5906.2011.01568.x Suarez-Almazor, M., Newman, C., Hanson, J., & Bruera, E. (2002). Attitudes of terminally ill cancer patients about euthanasia and assisted suicide: predominance of psychosocial determinants and beliefs over symptom distress and subsequent survival. Journal of Clinical Oncology, 20(8), 2134–2141. https://doi.org/ 10.1200/JCO.2002.08.023
- 106. Sulmasy, D. P., Ely, E. W., & Sprung, C. L. (2016). Euthanasia and physician-assisted suicide. JAMA: Journal of the American Medical Association, 316, 1600. https://doi.org/10.1001/ jama.2016.14077 Sulmasy, D. P., Linas, B. P., Gold, K. F., & Schulman, K. A. (1998). Physician resource use and willingness to participate in assisted suicide. Archives of Internal Medicine, 158, 974–978. https://doi.org/10.1001/archinte.158.9.974 Tossani, E. (2013). The concept of mental pain. Psychother Psychosom, 82, 67–73. https://doi.org/10.1159/000343003 Vilches, L. (2001). On Eutanasia. Revista de Psicologia, X, 177–187. https://doi.org/10.5354/0719-0581.2001.18561 Wilson, K. G., Chochinov, H. M., McPherson, C. J., Skirko, M. G., Allard, P., Chary, S., . . . Clinch, J. J. (2007). Desire for euthanasia or physician-assisted suicide in palliative cancer care. Health Psychology, 26(3), 314–323. https://doi.org/ 10.1037/0278-6133.26.3.314 Wilson, K., Scott, J., Graham, I., Kozak, J., Chater, S., Viola, R., . . . Curran, D. (2000). Attitudes of terminally ill patients toward euthanasia and physician-assisted suicide. Arch Intern Med, 160(16), 2454–2460. https://doi.org/10.1001/archinte.160. 16.2454 Wu, A., Wang, J. Y., & Jia, C. X. (2015). Religion and completed suicide: A meta-analysis. PLoS One, 10, e0131715. https://doi.
- 107. org/10.1371/journal.pone.0131715 Youngner, S. J., & Arnold, R. M. (2016). The Oxford handbook of ethics at the end of life. Oxford, UK: Oxford University Press.. Received August 3, 2017 Revision received November 16, 2017 Accepted January 23, 2018 Published online August 16, 2018 Miguel Ricou Faculty of Medicine University of Porto Alameda Prof. Hernâni Monteiro 4200-519 Porto Portugal [email protected] Miguel Ricou (PhD) is an Assistant Professor of Bioethics and of Pallia- tive Care, both at the Faculty of Medicine of Oporto University, and also an Assistant Professor of Psy- chopathology at Portucalense University. He acts as President of the Ethics Committee of the Order of Portuguese Psychologists and sup- ports the EFPA Board of Ethics in form of the Portuguese Representa- tive. Tony Wainwright is a clinical psy- chologist with many years experience working in the UK National Health Service. His main areas of clinical practice have been with older people
- 108. and those with long-term mental ill health. He has had a long-standing interest in the field of professional ethics and its links with human rights. He also has a strong com- mitment to the field of applied psy- chology in public health and how the way we are damaging the environ- ment leading to climate change and biodiversity loss has impacted on social justice and human rights. He is the deputy academic director on the University of Exeter Doctorate in Clinical Psychology Programme where he teaches on ethics, leader- ship and human rights. European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe Publishing 256 M. Ricou & T. Wainwright, The Psychology of Euthanasia T hi s do cu m en t i s co
- 111. in te nd ed s ol el y fo r t he p er so na l u se o f t he in di vi du
- 113. Death Studies, 38: 582–588, 2014 Copyright © Taylor & Francis Group, LLC ISSN: 0748-1187 print/1091-7683 online DOI: 10.1080/07481187.2013.820228 The Role of and Challenges for Psychologists in Physician Assisted Suicide Shara M. Johnson, Robert J. Cramer, Mary Alice Conroy, and Brett O. Gardner Department of Psychology, Sam Houston State University, Huntsville, Texas, USA Physician assisted suicide (PAS) poses complex legal and ethical dilemmas for practicing psychologists. Since the passage of the Oregon Death with Dignity Act in 1997, Montana and Washington have passed similar legislation. Despite the law requiring competence evaluations by medical and psychological professionals, existing psycholegal literature inadequately addresses the role of psychologists in the PAS process. This article reviews legal statutes and analyzes ethical dilemmas psychologists may face if involved. We con- sider competence both generally and in the context of PAS. Suggestions are made for psychologists completing competence assessments and future directions to improve com- petence assessments for PAS are provided. Human beings possess greater lifespans than at any point in history due to advancements in modern medicine and technology. The average lifespan in 1900 was 47.3 years; by 1997 it was 76.5 (Kramarow, Lentzner, Rooks, Weeks,
- 114. & Saydah, 1999). The trend has continued: From 1980 to 2005, life expectancy increased by nearly four years (National Center for Health Statistics, 2010). Although living longer is generally viewed as a blessing, society is witnessing increased rates of chronic disease and termi- nal illness as a result (National Center for Health Statistics, 2010). Advances in medical technology can often postpone these deaths, but many view a life pro- longed by dialysis, ventilators, and feeding tubes as unde- sirable (Sears & Stanton, 2001). In the United States, people are increasingly express- ing an interest in controlling the way their lives end should they be diagnosed with a terminal illness or chronic con- dition that yields a poor quality of life (Cerminara & Perez, 2000). As a result, every state has legalized advance directives, which allow individuals to specify the circum- stances in which particular life sustaining treatments may be refused or withdrawn, ensuring that their wishes are respected in the event they are rendered incompetent to make their own medical decisions (Sears & Stanton, 2001; Werth, Lewis, & Richmond, 2009). Physician assisted suicide (PAS) and euthanasia are alternative end-of-life decisions. PAS and euthanasia both hasten the death of an individual, but the two con- cepts meaningfully differ in the role of the physician (Cerminara & Perez, 2000; Sears & Stanton, 2001). Physicians carrying out a request for PAS provide indi- viduals with the means, generally prescription medica- tion, to end their life; individuals decide if and when to use the means. Euthanasia indicates cases in which the physician administers the lethal dose of medication with the intention of killing the patient (Cerminara & Perez, 2000; Sears & Stanton, 2001).
- 115. This review examines PAS from both legal and ethical perspectives, and discusses issues related to assessment of competence in patients requesting PAS in an effort to clarify the role and duties of psychologists participating in competence evaluations. The practice of PAS is widely considered to be a criminal offense; however, the practice is currently legal in Oregon, Washington, and Montana (Oregon Death with Dignity Act [ODDA], 1995; Washington Death with Dignity Act [WDDA], 2008; Baxter v. Montana, 2009). PAS is also a highly controver- sial topic from an ethical standpoint and the duties of psychologists involved in the process remain unclear. Thus, we present arguments regarding the rationality of suicide as a framework for understanding the debate that surrounds the acceptability of PAS. We include a review Received 29 September 2012; accepted 6 June 2013. Address correspondence to Shara M. Johnson, Department of Psychology, Sam Houston State University, Huntsville, TX 77341. E-mail: [email protected] THE ROLE OF AND CHALLENGES FOR PSYCHOLOGISTS 583 of the ambiguous ethical obligations of psychologists involved in PAS. In addition, guidelines for psychologists tasked with determining competence are critiqued, and we offer practical suggestions for completing the evalua- tion. Lastly, we identify areas for future research to improve PAS competence evaluations.
- 116. PHYSICIAN ASSISTED SUICIDE LEGISLATION: CRITERIA AND THE ROLE OF MENTAL HEALTH PROFESSIONALS In 1994, voters passed the ODDA (1995), which became available for use at the end of 1997 following a failed attempt to have the law repealed (Werth, Benjamin, & Farrenkopf, 2000). To qualify for PAS, an individual must be (a) a resident of Oregon (Oregon Revised Statute [ORS] 127.860 § 3.10), (b) at least 18 years old (ORS 127.805 § 2.01), (c) terminally ill, which two physicians agree will result in death within 6 months (ORS 127.820 § 3.02), and (d) making an informed decision (ORS 127.830 § 3.04). Furthermore, (e) the individual must make three requests to his or her attending physician, two oral and one written (ORS 127.840 § 3.06). The oral requests must be made at least 15 days apart, and an additional waiting period of 48 hr must pass between the written request and the prescrip- tion (ORS 127.850 § 3.08). Lastly, (f) the physician must offer to stop the process following the second oral request, which the individual must refuse (ORS 127.845 § 3.07). According to ODDA, to receive the life ending pre- scription, the patient must be considered to be making an “informed decision,” which is based on appreciation of the relevant facts and after being fully informed by the attending physician of: a) his or her medical diagnosis; b) his or her prognosis; c) the potential risks associated with taking the medication to be prescribed; d) the probable result of taking the medi- cation to be prescribed; and e) the feasible alternatives, including, but not limited to, comfort care, hospice care, and pain control. (ORS 127.800 § 1.01.7)
- 117. As the law is written, a mental health professional should only become involved in requests for PAS when either the attending or consulting physician believes the patient is “suffering from a psychiatric or psychological disorder or depression causing impaired judgment” and makes a “counseling referral” (ORS 127.825 § 3.03). It is up to “the person performing the counseling” to deter- mine that the patient is no longer suffering from the psy- chological disorder causing impaired judgment and capable of continuing with PAS. However, the definition of capable provided by the ODDA, “the ability to make and communicate health care decisions to health care providers” is too vague to serve as a guide for psycholo- gists asked to make such a determination (ORS 127.800 § 1.01; Werth et al., 2000). Guidelines do not exist and no recent court cases have clarified what constitutes decisional competency in PAS (Werth et al., 2000). Two other states have followed Oregon. In 2008, Washington voted to adopt an assisted suicide law (WDDA, 2008). In 2009, the District Court of Montana held that state residents’ constitutional rights of individ- ual privacy and human dignity grant the right of a “com- petent, terminally ill patient to die with dignity” (Montana Death with Dignity Act [MDDA], 2009). The Montana Court went on to permit patients to use the assistance of their physician in obtaining a prescription for a lethal dose of medication, but specified that the patient is responsible for deciding to self-administer the medication and induce death (Baxter v. Montana, 2009). ARGUMENTS FOR AND AGAINST PAS Understanding variant perspectives on suicide itself is necessary to fully evaluate the ethical issues involved in
- 118. PAS. From a medical model, suicidal ideation is com- monly considered symptomatic of mental illness and irra- tionality (Sullivan, Ganzini, & Younger, 1998). As proof, thoughts of death are listed among diagnostic criteria for depression in the Diagnostic and Statistical Manual (4th ed., text rev.; American Psychiatric Association, 2000), much clinical literature is devoted to assessing and pre- venting suicide (e.g., Bryan, Corso, Neal-Walden, & Rudd, 2009; Cukrowicz, Wingate, Driscoll, & Joiner, 2004; Kleespies & Dettmer, 2000; Wingate, Joiner, Walker, Rudd, & Jobes, 2004), and numerous organizations (i.e., American Association of Suicidology, American Foundation for Suicide Prevention, and International Association for Suicide Prevention) are committed to pre- venting suicide (Silverman, 2000). Furthermore, the implication that suicidal ideation indicates incapacitating pathology extends into the legal arena and is used to jus- tify involuntary commitment and mental health treatment (Sullivan et al., 1998). Although a wide body of research on suicide exists, it focuses primarily on prediction and prevention; very little conceptualizes suicide as a rational alternative (Werth, 1998; Widiger & Rinaldi, 1983). This emphasis likely reflects a denial of circumstances that may render a life no longer worth living and common fears about death. Two arguments support suicide prevention. The first is the link between suicidal ideation and psychopathology (Widiger & Rinaldi, 1983). Indeed, presence of suicidal ideation results in a lower Global Assessment of Functioning score, which is a rating of psychological dys- function. Suicidal behavior also mimics four features common among mental disorders: the low base rate for suicide represents a deviation from normal behavior, it is viewed as undesirable by society, it is indicative of high levels of distress, and it impairs functioning in one or
- 119. more domains (Widiger & Rinaldi, 1983). The second is 584 S. M. JOHNSON ET AL. the ambivalence of the individual toward death. Individuals who are in, or seek, treatment during their suicidal crisis are perceived to be ambivalently committed to ending their own life and receptive toward intervention (Widiger & Rinaldi, 1983). Belief in an inherent right to autonomy and acknowl- edgement of the possibility that death can be a desirable alternative to life are arguments used by those who lobby for an acceptance of suicide (Silverman, 2000; Widiger & Rinaldi, 1983). Autonomy proponents believe that indi- viduals have the right to oversee their own goals and des- tinies, which includes the manner and timing of their death. They argue psychologists’ duty to commit or refer a patient who is experiencing suicidal ideation fully removes the autonomy from the patient so that the psy- chologist assumes control over the suicidal patient (Abeles & Barlev, 1999). They also point out that circum- stances may arise in which the individual experiences unbearable suffering or permanent impairment, and death would be a merciful relief (Silverman, 2000; Widiger & Rinaldi, 1983). From this perspective, there is little perceived difference between PAS and acceptable end-of-life alternatives, such as refusal or withdrawal of life sustaining treatment (Jamison, 2000). Opponents of PAS cite numerous concerns. One com- mon argument is that PAS would be unnecessary if termi- nally ill patients had adequate palliative care (Cerminara & Perez, 2000; Jamison, 2000; Rosenfeld, 2000). It is
- 120. argued that more effective pain management for termi- nally ill patients and additional social support for the patient and family should be developed. Another fre- quently cited argument against PAS is monetary; PAS is less expensive than extensive palliative treatment and might be more frequently used when medical resources are scarce (Rosenfeld, 2000). Furthermore, it has been theorized that should such a scarcity arise, PAS may be used more frequently with members of vulnerable soci- etal groups, such as minorities, individuals with disabili- ties, and those of low socioeconomic status (Rosenfeld, 2000). Lastly, there is fear that legalizing PAS will lead to a slippery slope in which euthanasia and assisted death for patients not suffering from a terminal illness also become legal (Rosenfeld, 2000). In fact, White and Callahan (2000) proposed that “the most disastrous long- term effect of legal PAS would be to legitimate suicide as a socially acceptable way of dealing with pain and suffer- ing of life and the end of life” (p. 333). THE ROLE OF PSYCHOLOGISTS The legal statutes recommend that a psychologist become involved in PAS when there are concerns regarding the patient’s decisional capacity due to the presence of psy- chopathology, such as depression (ODDA, 1995; WDDA, 2008; MDDA, 2009). There appears to be a consensus that the training psychologists receive in assessment, psychopathology, and cognitive impairment qualifies them to assist in determining whether a patient is capable to consent to PAS (Farberman, 1997; Farrenkopf & Bryan, 1999; Werth et al., 2000; Werth et al., 2009). It has been proposed that psychologists with forensic training may be uniquely qualified to evaluate competence requests in PAS, given their training and experience with
- 121. issues related to competence and capacity (Ganzini, Leong, Fenn, Silva, & Weinstock, 2000). Indeed, a survey of forensic psychiatrists revealed that the majority had professional experience with competence evaluations and end-of-life decisions, with 74% having conducted compe- tence evaluations for individuals refusing life sustaining treatment, 54% having personally cared for a family member or close friend who was suffering from a termi- nal illness, and 67% having witnessed the suffering of a dying family member or friend (Ganzini et al., 2000). There is no consensus regarding the extent to which the psychologist should be involved in the process and the statutes provide no guidance aside from allowing for the assessment. According to Farrenkopf and Bryan (1999), when consulting on a case of PAS, the psychologist should first clarify the reason for the referral, which may be an evaluation of competence, but may also include treatment of a disorder and treatment designed to improve competence. In addition to performing the assessment, Farberman (1997) proposed that psycholo- gists serve as protectors of the patient’s rights and pro- vide support for the patient’s family. In a survey of Oregonian psychologists, further dis- agreement regarding the psychologist’s role was revealed. Sixty-two percent of those willing to perform the evalua- tion indicated they would take no further action after providing the referring physician with a report (Fenn & Ganzini, 1999). However, 28% reported they would sup- port the patient in completing the request, whereas 10% reported they would actively work to prevent the suicide (Fenn & Ganzini, 1999). ETHICAL CONSIDERATIONS FOR PSYCHOLOGISTS