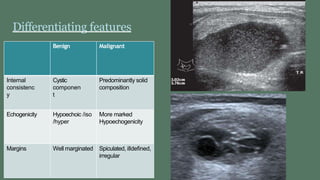
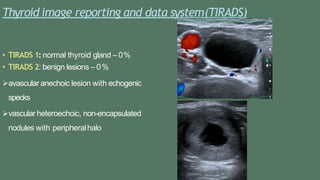
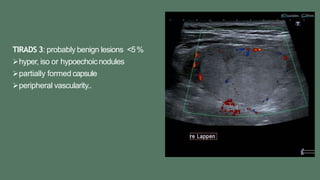
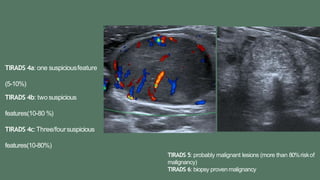
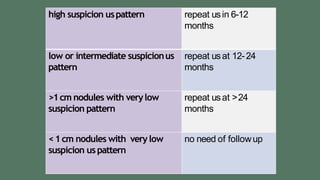
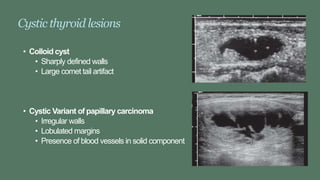
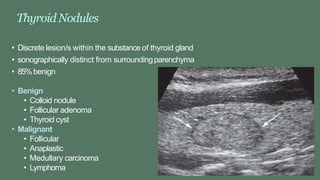
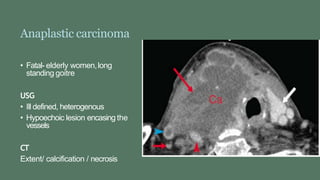
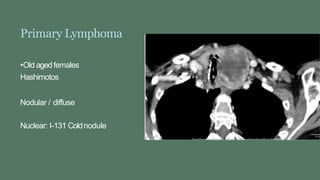
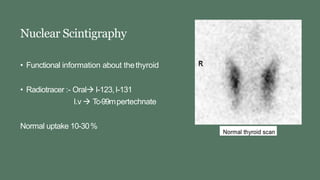
This document discusses the imaging of thyroid lesions using various modalities such as ultrasound, CT, MRI, and nuclear scintigraphy. It describes the appearance of common benign and malignant thyroid lesions on ultrasound, including features that help differentiate them. Newer techniques for thyroid imaging such as elastography, contrast-enhanced ultrasound, PET, perfusion CT, diffusion MRI, and magnetic resonance spectroscopy are also summarized.