Contents
• Overview ofAnatomy
• Supply of thyroid gland(arterial , venous, lymphatic)
• Surgical anatomy importance
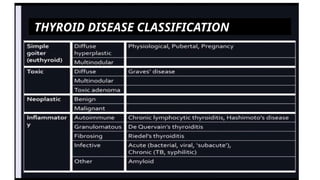
• Classification of thyroid disease
• Investigations for benign thyroid Disease
3.
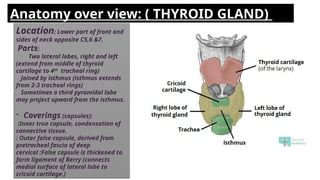
Location: Lower partof front and
sides of neck opposite C5,6 &7.
Parts:
Two lateral lobes, right and left
(extend from middle of thyroid
cartilage to 4th
tracheal ring)
Joined by isthmus (isthmus extends
from 2-3 tracheal rings)
Sometimes a third pyramidal lobe
may project upward from the isthmus.
- Coverings (capsules):
:Inner true capsule, condensation of
connective tissue.
: Outer false capsule, derived from
pretracheal fascia of deep
cervical :False capsule is thickened to
form ligament of Berry (connects
medial surface of lateral lobe to
cricoid cartilage.)
Anatomy over view: ( THYROID GLAND)
4.
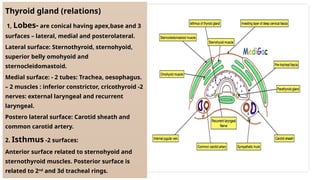
Thyroid gland (relations)
1,Lobes- are conical having apex,base and 3
surfaces – lateral, medial and posterolateral.
Lateral surface: Sternothyroid, sternohyoid,
superior belly omohyoid and
sternocleidomastoid.
Medial surface: - 2 tubes: Trachea, oesophagus.
– 2 muscles : inferior constrictor, cricothyroid -2
nerves: external laryngeal and recurrent
laryngeal.
Postero lateral surface: Carotid sheath and
common carotid artery.
2. Isthmus -2 surfaces:
Anterior surface related to sternohyoid and
sternothyroid muscles. Posterior surface is
related to 2nd
and 3d tracheal rings.
5.
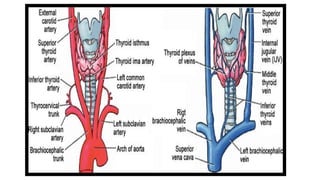
Arterial supply:
1. Superiorthyroid artery
2. Inferior thyroid artery
3. Thyroid Ima artery
Superior thyroid artery is closely
related to external laryngeal nerve.
Exernal lrygeal nerve.
Inferiorthyroid artery is closely
related to recurrent laryngeal nerve.
Surgical importance: Careful
Inferior thyroid artery ligation in
thyroid surgery.
Venous supply
3 pairs of veins:
1.Superior thyroid vein – ascend
along superior thyroid artery and
drains into the internal vein jugular
vein.
2.Middlle thyroid vein – directly
lateral drains into Internal jugular
→
vein. 3.Inferior thyroid vein
(variable):
Right – drainage >right or left
brachiocephalic Left-drainage let
→
vein brachiocephalic vein.
Thyroid gland Lymphatic drainage: Prelaryngeal, pretraheal and para-tracheal lymph nodes.
NERVE SUPPLY :
Principally from autonomic nervous system. Parasympathetic fibres –from vagus Sympathetic
■ ■
fibers -from superior, middle, and inferior ganglia of the sympathetic trunk Enter the gland along
7.
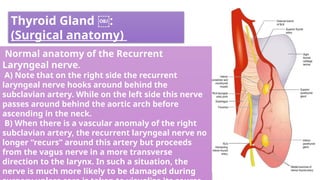
Thyroid Gland :
(Surgicalanatomy)
Normal anatomy of the Recurrent
Laryngeal nerve.
A) Note that on the right side the recurrent
laryngeal nerve hooks around behind the
subclavian artery. While on the left side this nerve
passes around behind the aortic arch before
ascending in the neck.
B) When there is a vascular anomaly of the right
subclavian artery, the recurrent laryngeal nerve no
longer “recurs” around this artery but proceeds
from the vagus nerve in a more transverse
direction to the larynx. In such a situation, the
nerve is much more likely to be damaged during
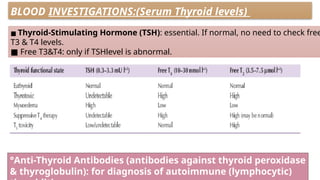
BLOOD INVESTIGATIONS:(Serum Thyroidlevels)
■ Thyroid-Stimulating Hormone (TSH): essential. If normal, no need to check free
T3 & T4 levels.
■ Free T3&T4: only if TSHlevel is abnormal.
°Anti-Thyroid Antibodies (antibodies against thyroid peroxidase
& thyroglobulin): for diagnosis of autoimmune (lymphocytic)
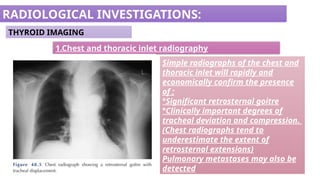
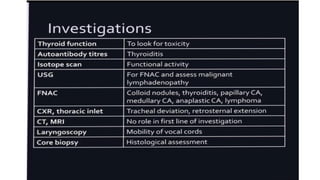
RADIOLOGICAL INVESTIGATIONS:
THYROID IMAGING
1.Chestand thoracic inlet radiography
Simple radiographs of the chest and
thoracic inlet will rapidly and
economically confirm the presence
of ;
°Significant retrosternal goitre
°Clinically important degrees of
tracheal deviation and compression.
(Chest radiographs tend to
underestimate the extent of
retrosternal extensions)
Pulmonary metastases may also be
detected
13.
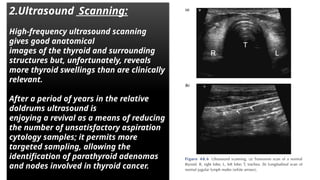
2.Ultrasound Scanning:
High-frequency ultrasoundscanning
gives good anatomical
images of the thyroid and surrounding
structures but, unfortunately, reveals
more thyroid swellings than are clinically
relevant.
After a period of years in the relative
doldrums ultrasound is
enjoying a revival as a means of reducing
the number of unsatisfactory aspiration
cytology samples; it permits more
targeted sampling, allowing the
identification of parathyroid adenomas
and nodes involved in thyroid cancer.
14.
Composition: Nodules canbe solid, mixed solid cystic,
entirely cystic, or spongiform. Among these, solid nodules have the
highest risk of malignancy.26 Spongiform nodules, characterized by
multiple microcystic areas forming more than 50% of the nodule,
have a high negative predictive value For malignancy.
Echogenicity: Nodules are iso, hypo, or hyperechoic if they are equal to, less
than, and more than the echogenicity of the Normal thyroid. Nodules are very
hypoechoic if they are less echogenic than the strap muscles.
Margins: They can be smooth, ill-defined (more than 50% contour is not made
out), lobulated, irregular, or can show overt extrathyroid extension into strap
muscles, trachea, esophagus, or larynx, which has the maximum risk
of malignancy. The presence of only capsular bulge, border
abutment, or loss of echogenic border is considered as
minimal extrathyroid extension, the clinical significance of which is controversial
Evaluation of Thyroid Nodules on
Ultrasonography
15.
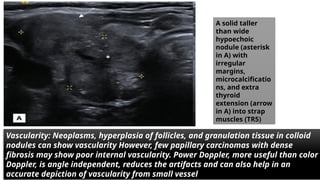
Vascularity: Neoplasms, hyperplasiaof follicles, and granulation tissue in colloid
nodules can show vascularity However, few papillary carcinomas with dense
fibrosis may show poor internal vascularity. Power Doppler, more useful than color
Doppler, is angle independent, reduces the artifacts and can also help in an
accurate depiction of vascularity from small vessel
A solid taller
than wide
hypoechoic
nodule (asterisk
in A) with
irregular
margins,
microcalcificatio
ns, and extra
thyroid
extension (arrow
in A) into strap
muscles (TR5)
16.
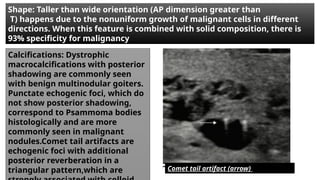
Shape: Taller thanwide orientation (AP dimension greater than
T) happens due to the nonuniform growth of malignant cells in different
directions. When this feature is combined with solid composition, there is
93% specificity for malignancy
Calcifications: Dystrophic
macrocalcifications with posterior
shadowing are commonly seen
with benign multinodular goiters.
Punctate echogenic foci, which do
not show posterior shadowing,
correspond to Psammoma bodies
histologically and are more
commonly seen in malignant
nodules.Comet tail artifacts are
echogenic foci with additional
posterior reverberation in a
triangular pattern,which are Comet tail artifact (arrow)
18.
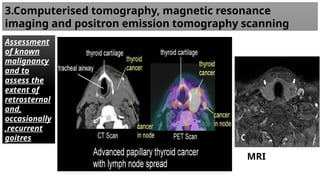
3.Computerised tomography, magneticresonance
imaging and positron emission tomography scanning
Assessment
of known
malignancy
and to
assess the
extent of
retrosternal
and,
occasionally
,recurrent
goitres
MRI
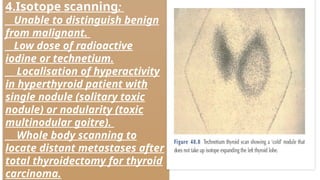
19.
4.Isotope scanning:
__Unable todistinguish benign
from malignant.
__Low dose of radioactive
iodine or technetium.
__ Localisation of hyperactivity
in hyperthyroid patient with
single nodule (solitary toxic
nodule) or nodularity (toxic
multinodular goitre).
__ Whole body scanning to
locate distant metastases after
total thyroidectomy for thyroid
carcinoma.
20.
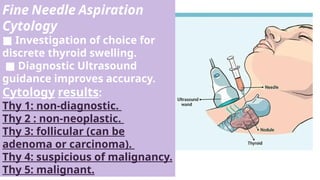
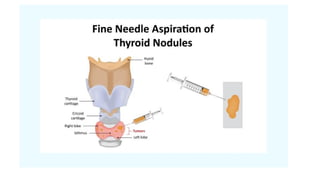
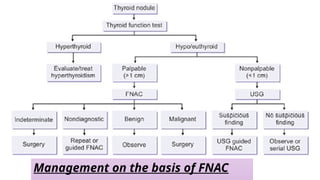
Fine Needle Aspiration
Cytology
■Investigation of choice for
discrete thyroid swelling.
■ Diagnostic Ultrasound
guidance improves accuracy.
Cytology results:
Thy 1: non-diagnostic.
Thy 2 : non-neoplastic.
Thy 3: follicular (can be
adenoma or carcinoma).
Thy 4: suspicious of malignancy.
Thy 5: malignant.
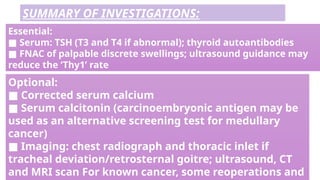
Optional:
■ Corrected serumcalcium
■ Serum calcitonin (carcinoembryonic antigen may be
used as an alternative screening test for medullary
cancer)
■ Imaging: chest radiograph and thoracic inlet if
tracheal deviation/retrosternal goitre; ultrasound, CT
and MRI scan For known cancer, some reoperations and
Essential:
■ Serum: TSH (T3 and T4 if abnormal); thyroid autoantibodies
■ FNAC of palpable discrete swellings; ultrasound guidance may
reduce the ‘Thy1’ rate
SUMMARY OF INVESTIGATIONS: