Download to read offline
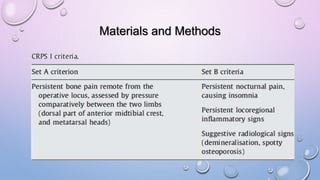
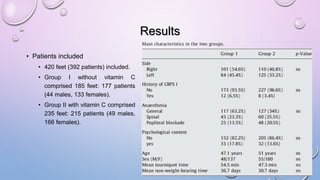
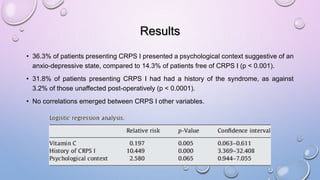


Vitamin C appears effective in preventing Complex Regional Pain Syndrome type 1 (CRPS 1) following foot and ankle surgery based on a prospective study. The study assessed 420 feet undergoing surgery, with 185 feet in a group that did not receive vitamin C and 235 feet in a group that received 1g of vitamin C daily for 45 days postoperatively. CRPS 1 occurred in 9.6% of the no vitamin C group but only 1.7% of the vitamin C group, indicating vitamin C may play a role in prevention. A history of CRPS 1 or anxious/depressive psychological traits increased the risk of developing postoperative CRPS 1. Larger prospective studies are still needed to confirm the findings.

![CRPS ppt sajad final final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/crpspptsajadautosaved-250921194258-ec8857be-thumbnail.jpg?width=640&height=640&fit=bounds)













































