Vraag 107 Dethalamus wordt gevasculariseerd door de arteria cerebri media Onjuist
3.
4.
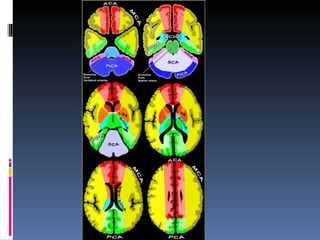
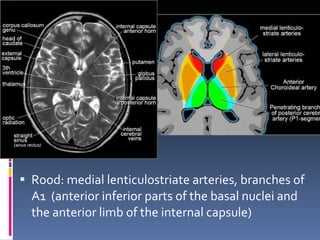
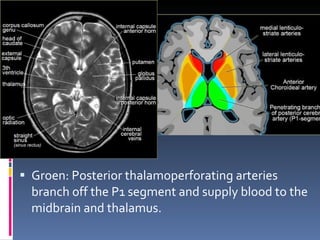
Rood: medial lenticulostriatearteries, branches of A1 ( anterior inferior parts of the basal nuclei and the anterior limb of the internal capsule)
5.
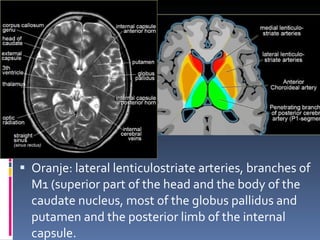
Oranje: lateral lenticulostriatearteries, branches of M1 (superior part of the head and the body of the caudate nucleus, most of the globus pallidus and putamen and the posterior limb of the internal capsule.
Vraag 107 Dethalamus wordt gevasculariseerd door de arteria cerebri media Onjuist
8.
Vraag 108 Devenae cerebri internae monden uit in de vena van Galeni Juist
9.
10.
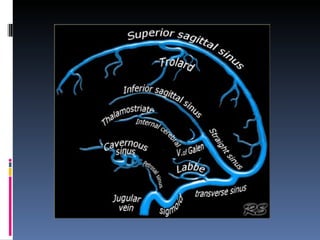
Veneuze afvloed Majordural sinuses: Superior sagittal sinus, transverse, straight and sigmoid sinuses. Cortical veins: Vein of Labbe, which drains the temporal lobe. Vein of Trolard, which is the largest cortical vein that drains into the superior sagittal sinus. Deep veins: Internal cerebral and thalamostriate veins. Cavernous sinus.
11.
Vraag 109 Indiener bij twijfel tussen een adenoom en een meningeoom (bijvoorbeeld in de regio van de sella) ossale hyperostose aanwezig is, pleit dit voor de diagnose meningeoom. Juist
12.
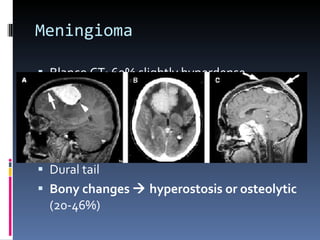
Meningioom Most commonextra-axial neoplasm Middle-aged women Parasagittal , convexities, cerebellopontine angle , olfactory groove 90% supratentorieel 1% extraduraal, sinonasal cavity
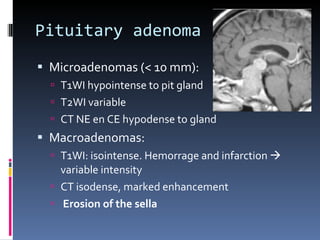
Pituitary adenoma Microadenomas(< 10 mm): T1WI hypointense to pit gland T2WI variable CT NE en CE hypodense to gland Macroadenomas: T1WI: isointense. Hemorrage and infarction variable intensity CT isodense, marked enhancement Erosion of the sella
15.
Vraag 109 Indiener bij twijfel tussen een adenoom en een meningeoom (bijvoorbeeld in de regio van de sella) ossale hyperostose aanwezig is, pleit dit voor de diagnose meningeoom. Juist
16.
Vraag 110 Hetcavum van Meckel bevat takken van de nervus abducens. Onjuist
17.
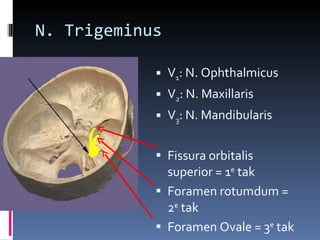
Cavum v Meckel= C avum trigeminale N. Trigeminus Ganglion Gasseri 1. Tentorium cerebelli superolaterally 2. The lateral wall of the sinus cavernosus superomedially 3. The clivus medially 4. The posterior petrous bone inferolaterally
18.
N. Trigeminus V1 : N. Ophthalmicus V 2 : N. Maxillaris V 3 : N. Mandibularis Fissura orbitalis superior = 1 e tak Foramen rotumdum = 2 e tak Foramen Ovale = 3 e tak
19.
Vraag 110 Hetcavum van Meckel bevat takken van de nervus abducens. Onjuist
20.
Vraag 111 Eenvan de typische kenmerken van pilocytaire astrocytomen is de neiging zich te verspreiden via de subarachnoïdale ruimte (zogenaamde ‘seeding’). Onjuist
21.
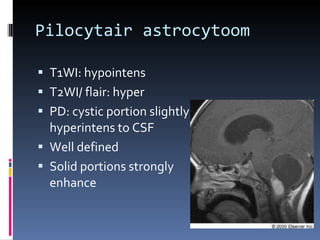
Pilocytair astrocytoom GradeI astrocytic tumor Peak age 0-20 years Most common intratentorial neoplasm in children Benign 60% in posterior fossa, less common optic pathways and hypothalamus Typical cystic (mural nodule), in older patients frequently solid
22.
Pilocytair astrocytoom T1WI:hypointens T2WI/ flair: hyper PD: cystic portion slightly hyperintens to CSF Well defined Solid portions strongly enhance
23.
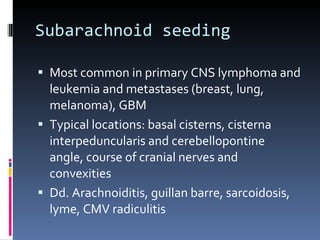
Subarachnoid seeding Mostcommon in primary CNS lymphoma and leukemia and metastases (breast, lung, melanoma), GBM Typical locations: basal cisterns, cisterna interpeduncularis and cerebellopontine angle, course of cranial nerves and convexities Dd. Arachnoiditis, guillan barre, sarcoidosis, lyme, CMV radiculitis
24.
Vraag 111 Eenvan de typische kenmerken van pilocytaire astrocytomen is de neiging zich te verspreiden via de subarachnoïdale ruimte (zogenaamde ‘seeding’). Onjuist
25.
Vraag 112 Opeen MRI-hersenen van een HIV-positieve patiënt ziet u een massa. U twijfelt tussen de diagnose toxoplasmose en lymfoom. Op een aanvullende blanco CT-hersenen is de massa hyperdens. Dit pleit voor de diagnose lymfoom. Juist
26.
Leading diagnoses inpatients with advanced AIDS who have “Mass Lesions” : Toxoplasma encephalitis 50% of all brain lesions in AIDS patients. Primary CNS Lymphoma (EBV) 30% of all brain lesions in AIDS patients
27.
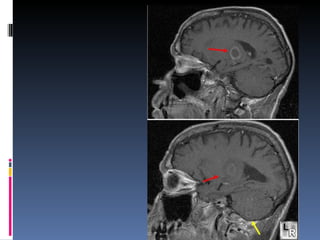
Toxoplasma encephalitis Thin-walledring-enhancing lesions, surrounding edema; rarely diffuse encephalitis Multiple lesions 80% Usually hyperintense with hypointense rim on T2 (can have decreased signal in central areas from calcium and hemorrhage) Basal Ganglia, G/W junction; parietal, frontal, thalamus More likely to appear in posterior fossa than Primary CNS lymphoma < 4 cm
28.
29.
Lymphoma & AIDSRing-enhancing lesions (multiple in 50%), little surrounding edema Variable signal on T2; iso/hypo on T1 High density masses on non-contrast CT scan Can be > 4cm Homogeneous enhancement (behalve wanneer necrotisch) Prediliction for basal ganglia, cerebellar hemispheres, thalamus, brain stem, corpus callosum and subependymal. More likely to cross corpus callosum than TE
30.
Vraag 112 Opeen MRI-hersenen van een HIV-positieve patiënt ziet u een massa. U twijfelt tussen de diagnose toxoplasmose en lymfoom. Op een aanvullende blanco CT-hersenen is de massa hyperdens. Dit pleit voor de diagnose lymfoom. Juist
31.
Vraag 113 Eenintracerebraal hematoom van 3 dagen oud heeft ten opzichte van het overige hersenparenchym een hoog signaal op T1-gewogen MRI-opnamen. Juist
32.
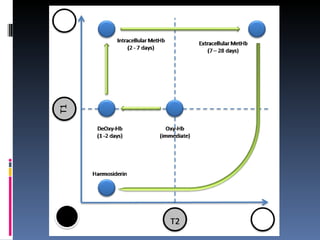
As a hematome ages,hemoglobin changes through several forms oxyhemoglobin, deoxyhemoglobin, and methemoglobin before the RBCs are broken down into ferritin and hemosiderin. Five distinct stages of hemorrhage can be defined Uitleg: http://emedicine.medscape.com/article/344973-overview#aw2aab6b5 Stages of hemorrhage
33.
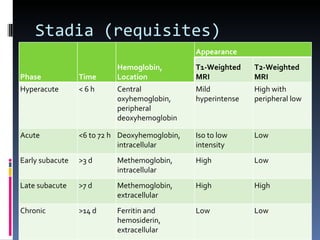
Stadia (requisites) PhaseTime Hemoglobin, Location Appearance T1-Weighted MRI T2-Weighted MRI Hyperacute < 6 h Central oxyhemoglobin, peripheral deoxyhemoglobin Mild hyperintense High with peripheral low Acute <6 to 72 h Deoxyhemoglobin, intracellular Iso to low intensity Low Early subacute >3 d Methemoglobin, intracellular High Low Late subacute >7 d Methemoglobin, extracellular High High Chronic >14 d Ferritin and hemosiderin, extracellular Low Low
34.
35.
Vraag 113 Eenintracerebraal hematoom van 3 dagen oud heeft ten opzichte van het overige hersenparenchym een hoog signaal op T1-gewogen MRI-opnamen. Juist Vervallen
36.
Vraag 114 Eénvan de voorkeurslokalisaties van DAI (diffuse axonal injury) betreft het corpus callosum. Juist
37.
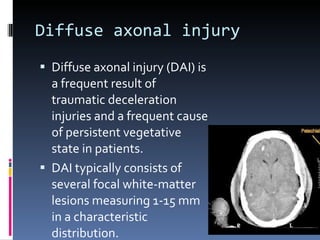
Diffuse axonal injuryDiffuse axonal injury (DAI) is a frequent result of traumatic deceleration injuries and a frequent cause of persistent vegetative state in patients. DAI typically consists of several focal white-matter lesions measuring 1-15 mm in a characteristic distribution.
38.
Locations Gray-white junctionCorpus callosum (body en splenium) Brain stem Superior cerebellar peduncle Internal capsule
39.
Vraag 114 Eénvan de voorkeurslokalisaties van DAI (diffuse axonal injury) betreft het corpus callosum. Juist
40.
Vraag 115 Hetcerebellum is minder goed bestand tegen hypoxie dan het cerebrum. Onjuist
41.
Onderscheid hypoxie /anoxieAnoxia: Near-complete absence of oxygen for more than 5 min (cardiac arrest, prolonged seizures, hanging, CO inhalation) Hypoxia: Partial but more prolonged hypoxemia
42.
Anoxie Na anoxiezijn de metabool actieve delen van het brein het meest aangedaan (basale ganglia, hippocampus) Verminderde differentiatie tussen basale ganglia en capsula interna
43.
Hypoxia Damage tothose portions of the brain that are farthest from the heart. Basale ganglia en hippocampi relatief gespaard Edema at gray-white junctions
44.
Vraag 115 Hetcerebellum is minder goed bestand tegen hypoxie dan het cerebrum. Onjuist
45.
Vraag 116 Opeen MRI-hersenen twijfelt u tussen een subduraal empyeem en een subduraal hygroom. Op aanvullende diffusie-gewogen (DWI) opnamen heeft de laesie een hoog signaal en op de apparent diffusion coëfficiënt (ADC) opnamen een laag signaal. Het beeld past het best bij een subduraal hygroom. Onjuist
46.
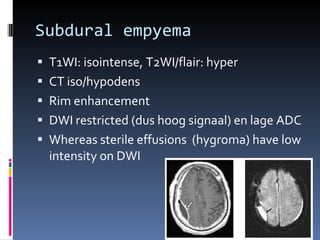
Subdural empyema T1WI:isointense, T2WI/flair: hyper CT iso/hypodens Rim enhancement DWI restricted (dus hoog signaal) en lage ADC Whereas sterile effusions (hygroma) have low intensity on DWI
47.
Vraag 116 Opeen MRI-hersenen twijfelt u tussen een subduraal empyeem en een subduraal hygroom. Op aanvullende diffusie-gewogen (DWI) opnamen heeft de laesie een hoog signaal en op de apparent diffusion coëfficiënt (ADC) opnamen een laag signaal. Het beeld past het best bij een subduraal hygroom. Onjuist
48.
Vraag 117 Eentypisch kenmerk van een intracerebraal abces is, dat dit wordt omgeven door relatief weinig oedeem. Onjuist
49.
Brain abscess Mostoften result of hematogenous dissemination Cardiac, drug abuse, pulmonary infection, sepsis Of direct: Trauma (penetrating injury, otitis, sinusitis Meestal frontal and parietal lobes Gray-white matter junction (in hamatogenous spread) Substantial surrounding edema
50.
Vraag 117 Eentypisch kenmerk van een intracerebraal abces is, dat dit wordt omgeven door relatief weinig oedeem. Onjuist
Editor's Notes
#7 Anterior Choroideal artery (AchA in blue)) The territory of the AChA is part of the hippocampus, the posterior limb of the internal capsule and extends upwards to an area lateral to the posterior part of the cella media. Originates from the internal carotid artery , though it also rarely arises from the middle cerebral artery .
#23 ilocytic astrocytoma. Sagittal postcontrast T1W MR image demonstrates the classic “cyst and nodule” appearance of a pilocytic astrocytoma in the posterior fossa. Thin rim enhancement is seen involving the cyst wall.
#47 Figure 3: Axial post-contrast T1WI shows ring enhancement of the right subdural fluid collection (arrow) with associated meningeal enhancement. Figure 4: Axial diffusion weighted images shows increased signal of the right subdural fluid collection (arrow) with low apparent diffusion coefficient.




![Neurovragen deel 2[1]](https://cdn.slidesharecdn.com/ss_thumbnails/neurovragendeel21-111013123109-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)









![Vgt ge voorjaar_2011_deel_1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/vgtgevoorjaar2011deel11-111013123358-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)





![Nuirooefenen vgt[1]](https://cdn.slidesharecdn.com/ss_thumbnails/nuirooefenenvgt1-110415032149-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























