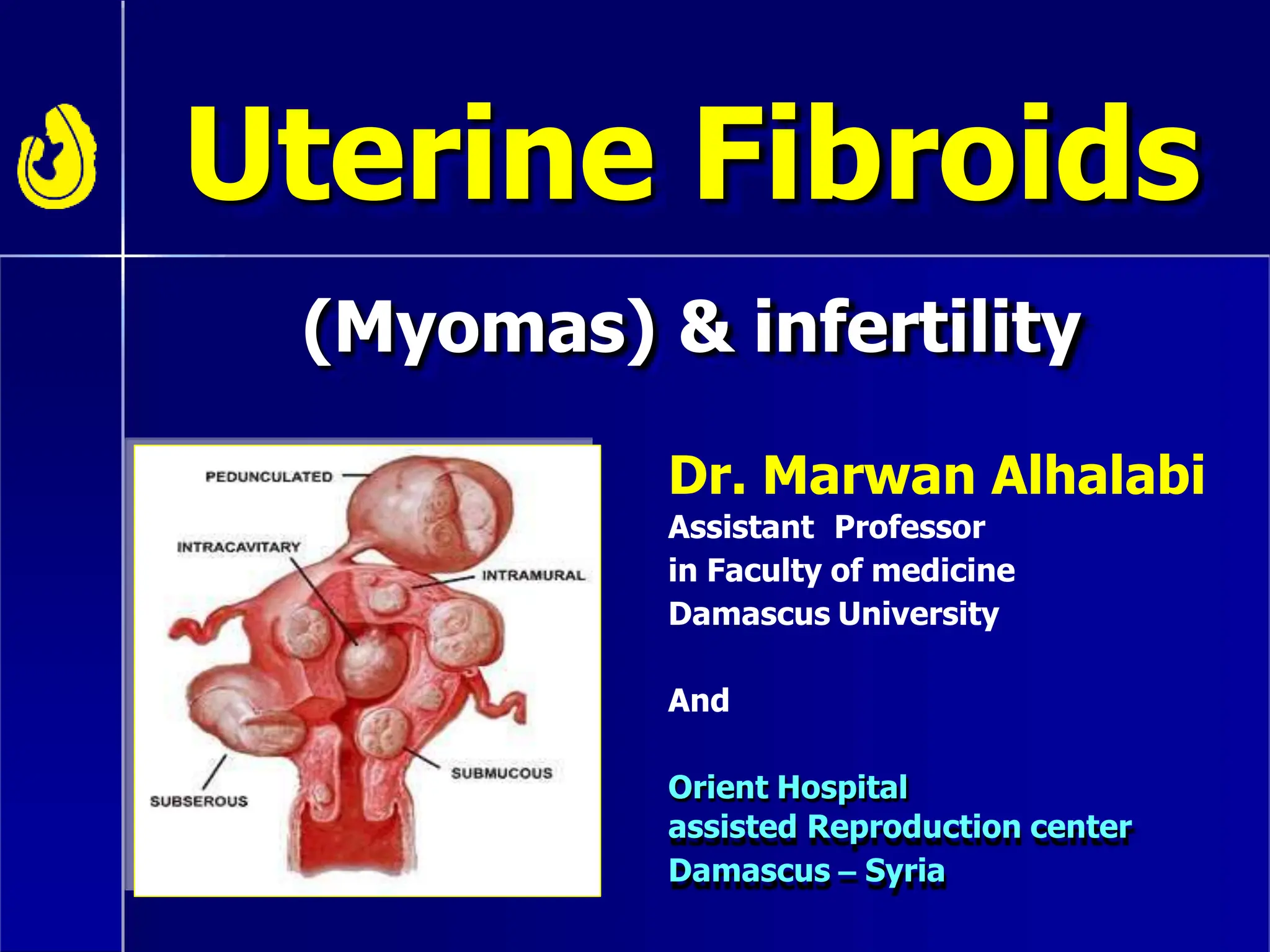
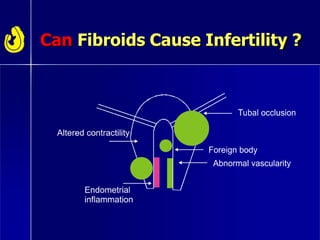
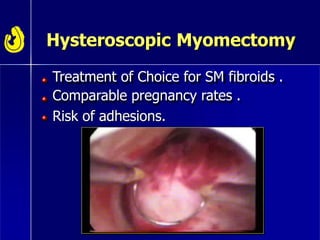
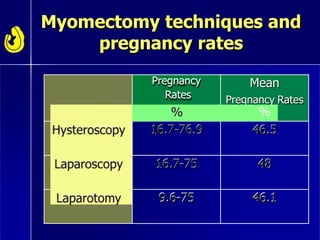
Uterine fibroids are common non-cancerous tumors that can affect fertility. While their exact effects are still being established, submucosal fibroids which distort the uterine cavity have been shown to decrease pregnancy rates. Myomectomy surgery to remove fibroids, especially those that are submucosal, can improve fertility outcomes by halving miscarriage risks and increasing pregnancy rates to similar levels as women without fibroids. The optimal treatment depends on factors like fibroid location, size and number, as well as the patient's age and fertility desires.