Downloaded 29 times
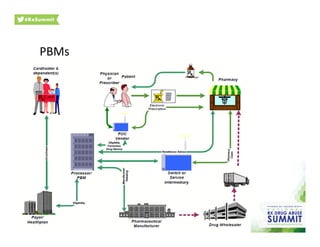

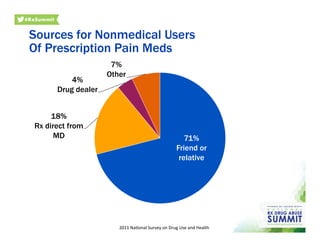
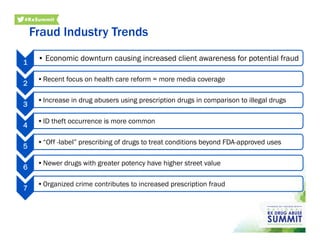

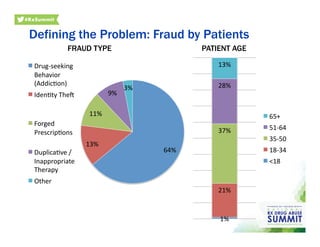
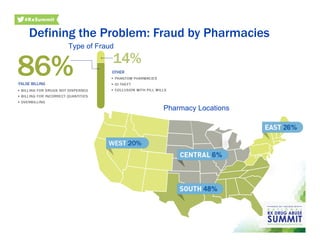

This document summarizes a presentation on using prescription drug data to limit misuse and abuse by third-party payers. The presentation features speakers from myMatrixx and Express Scripts discussing how data from sources like prescription drug monitoring programs, the DEA, NPPES, proprietary databases, and pharmaceutical manufacturers can be mined and analyzed to identify problematic prescribing patterns, problem geographic areas, and individual doctors who may be recklessly prescribing controlled substances. The goal is to organize collaboration between private and public agencies to help address the epidemic of prescription drug abuse.























































































