Download to read offline













































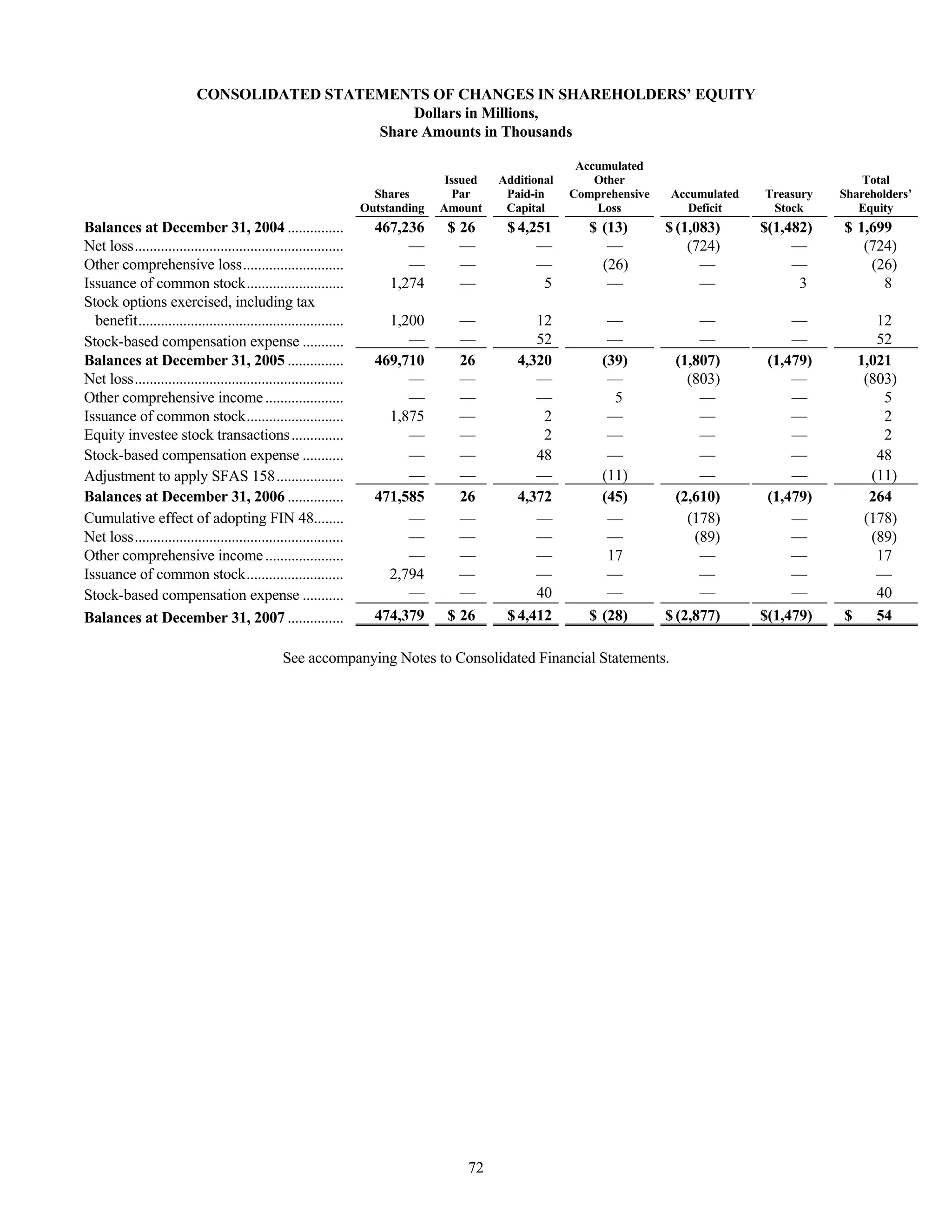























This document is Tenet Healthcare Corporation's annual report on Form 10-K for the fiscal year ended December 31, 2007. It provides information on Tenet's business operations including: 1) At the end of 2007, Tenet operated 57 general hospitals with a total of 15,244 licensed beds across 12 states. 2) In 2007, Tenet streamlined its regional structure and made strategic acquisitions and divestitures of hospitals. 3) Going forward, Tenet will focus on the 56 general hospitals that will remain after planned divestitures and new hospital construction projects are completed. These hospitals generated over 97% of Tenet's revenues.


































































































