DEFINITIONS
Traumatic Brain Injuryis an insult to the brain caused by
an external physical force
Diffuse Axonal Injury the tearing and shearing of
microscopic brain cells
Acquired Brain Injury is an insult to the brain that has
occurred after birth, for example; TBI, stroke, near
suffocation, infections in the brain, anoxia(an absence of
oxygen).
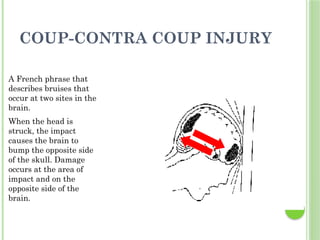
COUP-CONTRA COUP INJURY
AFrench phrase that
describes bruises that
occur at two sites in the
brain.
When the head is
struck, the impact
causes the brain to
bump the opposite side
of the skull. Damage
occurs at the area of
impact and on the
opposite side of the
brain.
5.
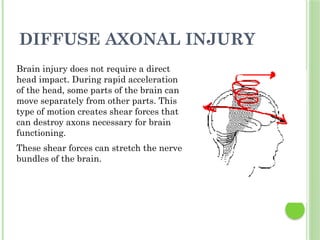
DIFFUSE AXONAL INJURY
Braininjury does not require a direct
head impact. During rapid acceleration
of the head, some parts of the brain can
move separately from other parts. This
type of motion creates shear forces that
can destroy axons necessary for brain
functioning.
These shear forces can stretch the nerve
bundles of the brain.
6.
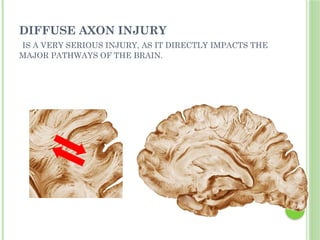
DIFFUSE AXON INJURY
ISA VERY SERIOUS INJURY, AS IT DIRECTLY IMPACTS THE
MAJOR PATHWAYS OF THE BRAIN.
7.
HEAD INJURY
TYPES OFHEAD
INJURIES
• Scalp lacerations
– Can bleed profusely
• Skull fractures
– Linear or depressed
• Linear is from a low velocity injury
– Simple, comminuted, or compound
– Closed or open
8.
HEAD INJURIES
Frontal fracture
•May see air in the forehead tissue, CSF coming out of
their nose
Orbital fracture
• Raccoon eyes, may have optic nerve injury
Parietal fracture
• Battle signs, facial paralysis
Basilar fracture
• CSF out ears, nose, battle signs, trouble hearing or
tinnitus, facial paralysis, conjugate gaze, vertigo.
9.
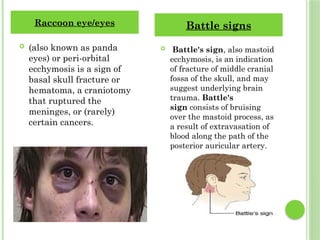
(also knownas panda
eyes) or peri-orbital
ecchymosis is a sign of
basal skull fracture or
hematoma, a craniotomy
that ruptured the
meninges, or (rarely)
certain cancers.
Battle's sign, also mastoid
ecchymosis, is an indication
of fracture of middle cranial
fossa of the skull, and may
suggest underlying brain
trauma. Battle's
sign consists of bruising
over the mastoid process, as
a result of extravasation of
blood along the path of the
posterior auricular artery.
Raccoon eye/eyes Battle signs
10.
HEAD INJURY
• Resultsfrom bleeding between the dura and the inner
surface of the skull
• Neurologic emergency!!!
• Venous or arterial origin
Epidural hematoma
Epidural hematoma
• Initial period of unconsciousness
• Headache
• Nausea, vomiting
• Focal findings
Classic signs include
11.
HEAD INJURY
Subduralhematoma
Occurs from bleeding between the dura mater and
arachnoid layer of the meningeal covering of the brain
Subdural hematoma
Acute subdural hematoma
Signs within 48 hours of the injury
Similar signs and symptoms to brain
tissue compression in increased ICP
Patient appears drowsy and confused
Ipsilateral pupil dilates and becomes fixed
12.
HEAD INJURY
IntracerebralHematoma
Occurs from bleeding within the parenchyma
Usually occurs within the frontal and temporal
lobes
Size and location of hematoma determine patient
outcome
Most of the time from a bullet (missile injury),
stabbing.
13.
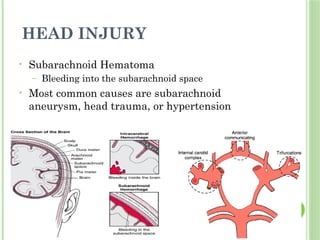
HEAD INJURY
• SubarachnoidHematoma
– Bleeding into the subarachnoid space
• Most common causes are subarachnoid
aneurysm, head trauma, or hypertension
14.
EFFECTS: PHYSICAL AND
COGNITIVE
14
PhysicalChanges
Headaches
Difficulty speaking
Blurry eyesight
Trouble hearing
Loss of energy
Change in sense of taste
or smell
Dizziness or trouble with
balance
Cognitive Changes
Difficulty concentrating
Trouble with attention
Forgetfulness
Difficulty making
decisions
Repeating things
15.
HEAD INJURY
DIAGNOSTIC STUDIESAND
COLLABORATIVE CARE
CT scan
• Best diagnostic test to determine craniocerebral trauma
MRI
PET
Transcranial Doppler studies
• Looking for vasospasm
Cervical spine x-ray
• You must see from C1 –C7 to see that they have no injury
Glasgow Coma Scale (GCS)
RX
Treatment principles
Prevent secondary injury in the brain
Timely diagnosis
Surgery if necessary
Assessment
Airway
Semi-Fowler’s positioning, really good oral care
Glasgow Coma Scale score
Neurologic status
Presence of CSF leak
Collaborative problem: Increased ICP
19.
ICP MONITORING
Indications
severe head injury (GCS < 9)
abnormal head CT
or
Coma >6 hrs
Intracranial hematoma requiring evacuation
Delayed neurologic deterioration from mild to
moderate (GCS>9) to severe (GCS < 8)
Requirement for prolonged ventilation
Pulmonary injury, surgery etc.
20.
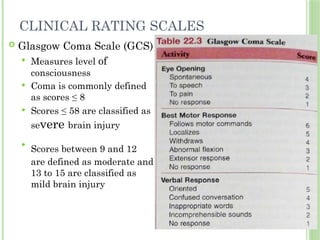
Glasgow ComaScale (GCS)
Measures level of
consciousness
Coma is commonly defined
as scores ≤ 8
Scores ≤ 58 are classified as
severe brain injury
Scores between 9 and 12
are defined as moderate and
13 to 15 are classified as
mild brain injury
CLINICAL RATING SCALES
23.
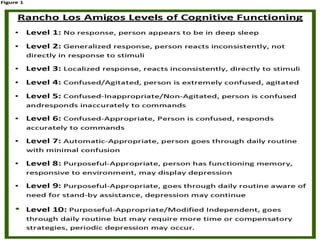
REHABILITATION
Rancho I,II, III
Sensory Stimulation.
Structured program of stimulation
Stimulating each sense
Educate family and significant others
PROM
Auditory stimulation
Visual stimulation
Olfactory stimulation
Vestibular stimulation


















![5 Head injury (1)[1]_425974386d4d442b6ce092649f8d5b41.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/5headinjury11425974386d4d442b6ce092649f8d5b41-250319190324-4867f9fb-thumbnail.jpg?width=640&height=640&fit=bounds)
![5 Head injury (1)[1]_425974386d4d442b6ce092649f8d5b41.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/5headinjury11425974386d4d442b6ce092649f8d5b41-250318200004-e6284666-thumbnail.jpg?width=640&height=640&fit=bounds)




















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



