Downloaded 16 times



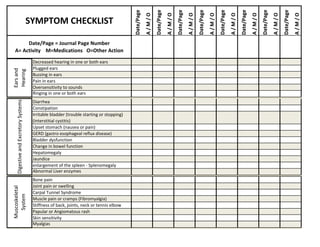
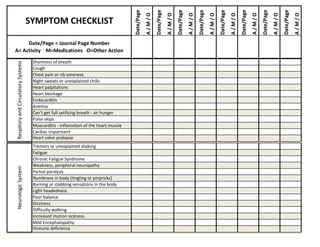
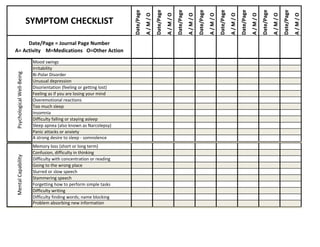
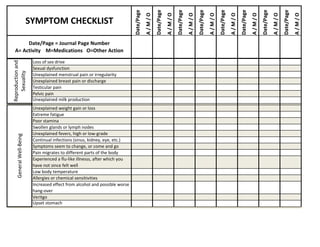
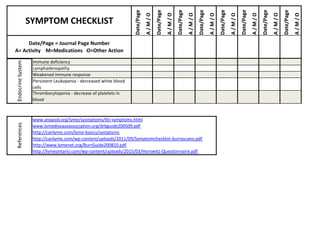

This document provides instructions for using a symptom checklist to track symptoms over time in order to identify patterns and the impact of activities, medications, and other factors. The checklist contains a comprehensive list of symptoms organized by body system. Users are directed to rate symptom severity on a scale, note the date and potential triggers, and reference their journal entries for additional details. Tracking symptoms over an extended period with this checklist and a personal journal can help users and healthcare providers determine effective treatment approaches.









![Standard+history++physical[1]](https://cdn.slidesharecdn.com/ss_thumbnails/standardhistoryphysical1-100422124650-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)
![Standard+history++physical[1]](https://cdn.slidesharecdn.com/ss_thumbnails/standardhistoryphysical1-100422124702-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
























































