Download as PDF, PPTX





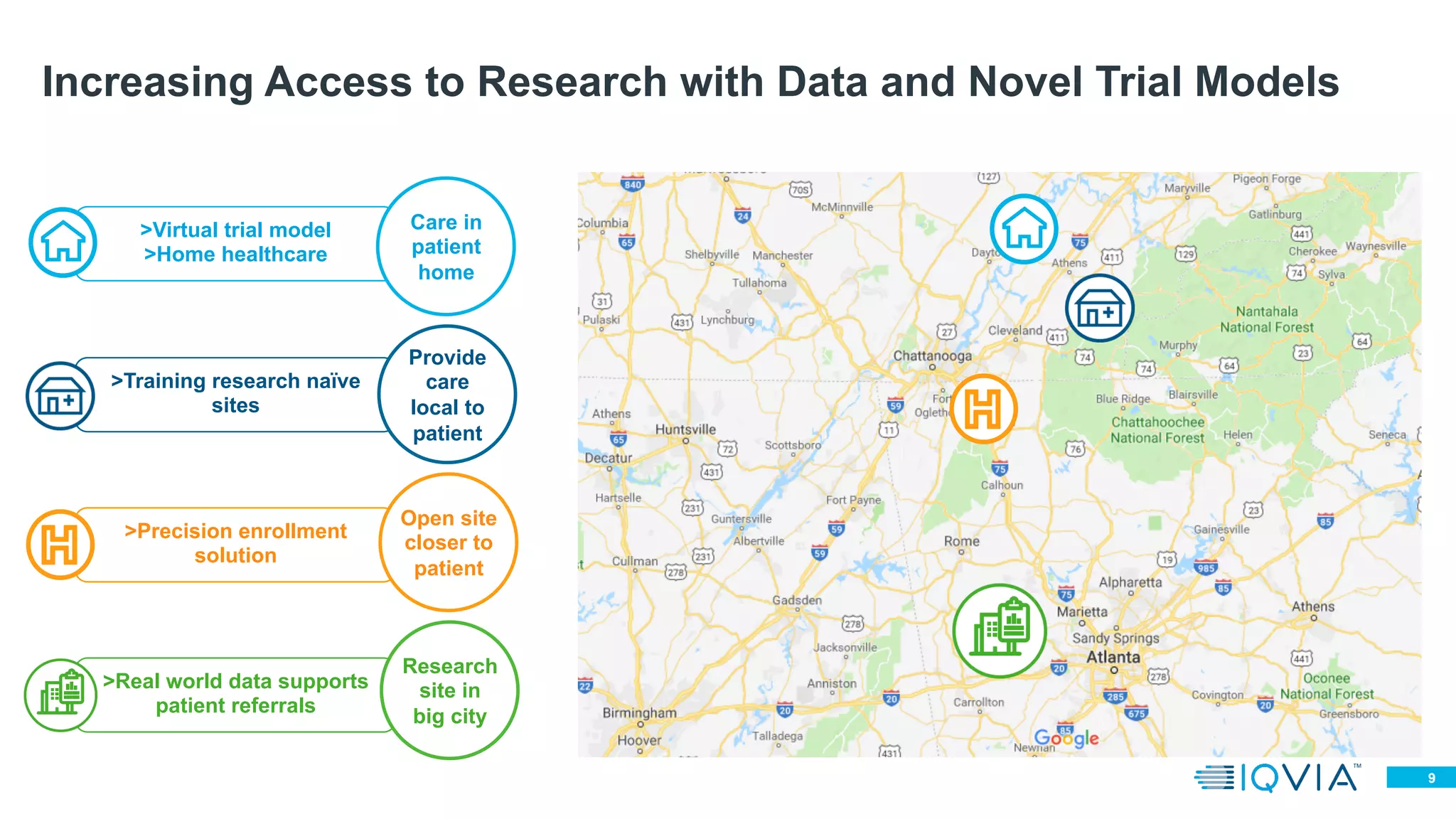




This document discusses the importance of increasing diversity in clinical trials, particularly for rare diseases, highlighting the need for representation across various demographics. It emphasizes innovative strategies to enhance trial access, such as establishing research infrastructure in sub-Saharan Africa and utilizing virtual trial models. Ultimately, improving access to clinical trials is crucial for developing effective treatments and benefiting diverse patient populations.























































































