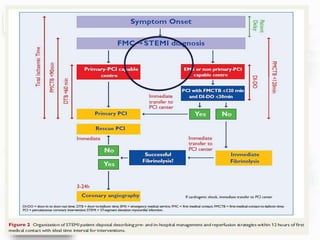
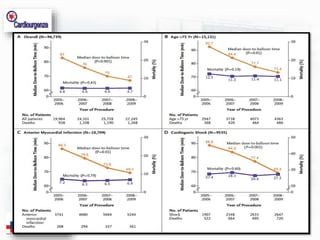
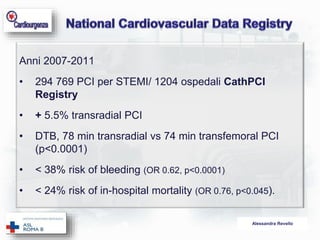
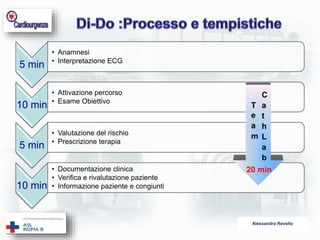
Il documento di Alessandra Revello analizza i ritardi nella terapia di riperfusione per infarti miocardici acuti con elevazione del tratto ST (STEMI), sottolineando l'importanza di ridurre i tempi dall'insorgenza dei sintomi alla terapia. Viene presentata un'analisi delle performance dei sistemi sanitario e ospedaliero coinvolti nel processo di riperfusione, evidenziando le misure necessarie per migliorare i tempi di trattamento e ridurre la mortalità intraospedaliera. È fondamentale un coordinamento efficace dei vari attori coinvolti, inclusi i servizi territoriali e ospedalieri, per ottimizzare i risultati clinici.