Downloaded 13 times







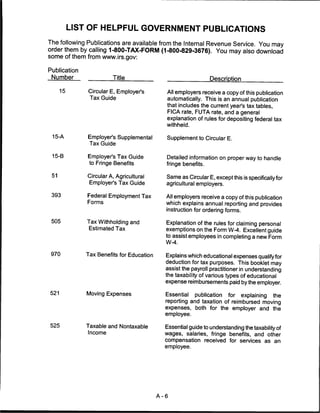



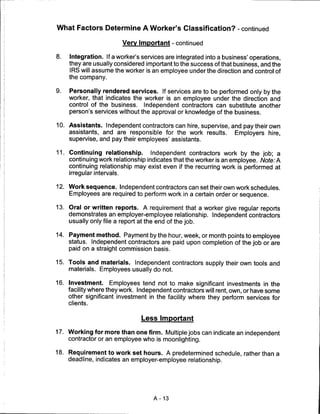
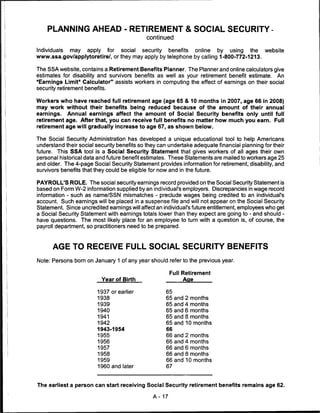




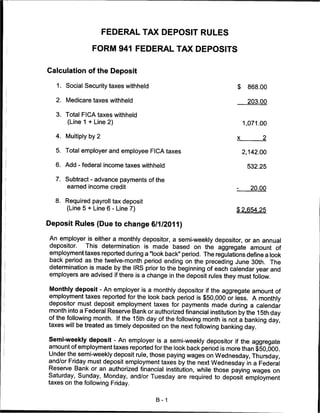

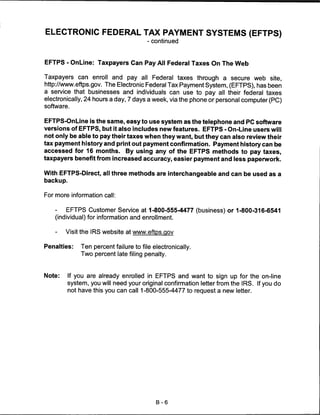

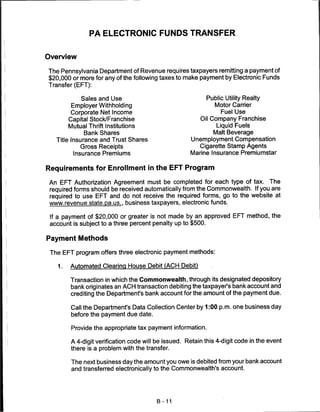
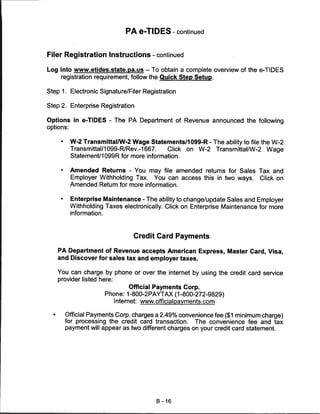
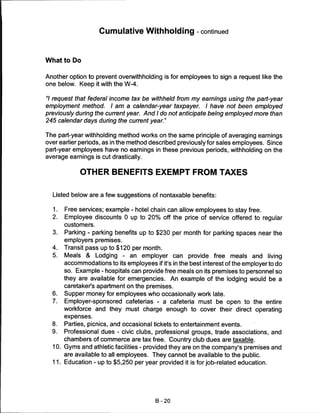
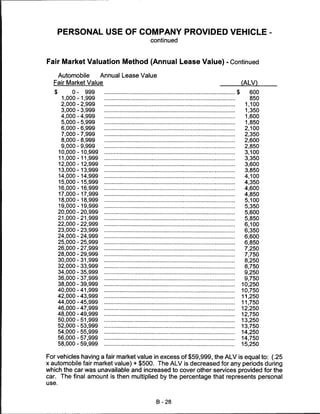
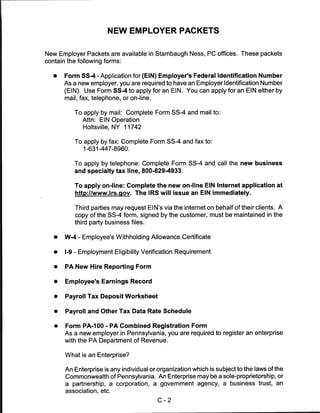
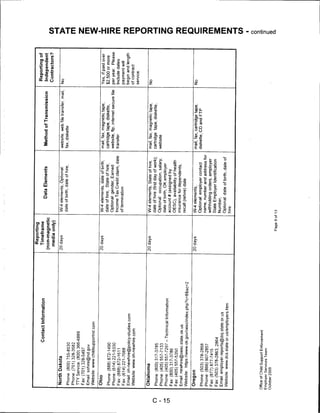
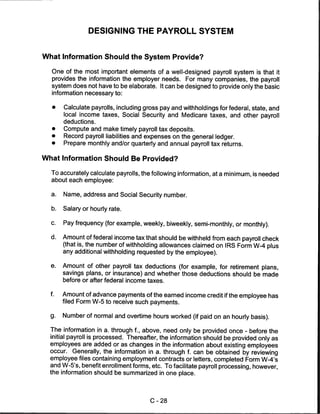
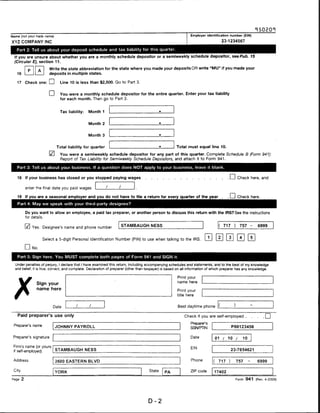
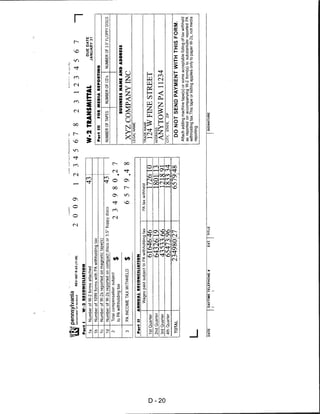
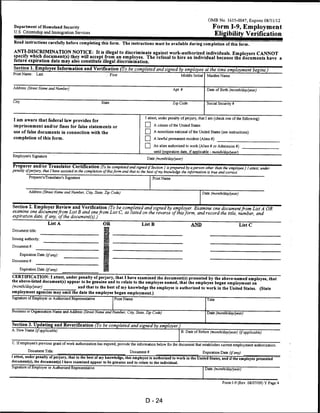
![Check the appropriate block(s) to indicate the tax(es) you will be paying by EFT. Enter the account number for each tax type. If you
select the ACH Debit option, the tax typefc) checked should fall under the bank account listed in Section 8 from which the
payments') will be drawn.
1 r~ Capital Stock/Franchise Tax File Box) Number
Loans Tax (AH 3 taxes reported on RCT-101)
Corporate Net Income Tax
File Box) Number
2. □ Utilities Gross Receipts Tax —
File Box) Number
3. Q Gross Receipts Telecommunication Taxes for
Intra-State, Inter-State, Mobile
—
File (Box) Number
4. □ Public Utility Realty Tax
File (Box) Number
5. □ Bank Shares Tax
Title Insurance & Trust Company Shares Tax
Bank Loans Tax
hie Box) Number
6. □ Mutual Thrift Institutions Tax —
File | Box) Number
7. Q Insurance Premiums Tax —
File (Box) Number
8. [] Marine Insurance Premiums Tax
EIN
9. n Liquid Fuels and Fuels Tax
Account Number
10. □ Motor Carriers Road Tax
Account Number
11. LJ IFTA - Motor Carriers
Account Number
12. □ Malt Beverage Tax
Account Number
13. C] Cigarette Stamp Agents
Account Number
14. □ Pari-Mutuel
Authorized Signature Information:
I certify the information provided on this form is true and correct and hereby authorize the PA Department of Revenue to use the
information herein in direct conjunction with the EFT program.
Print Name : Last First M.I. Title Date
Signature Telephone Mumber
Make a copy of this completed Authorization Agreement for your records. You may fax your completed Authorization Agreement to
(717) 787-0145, or mail it to the PA DEPARTMENT OF REVENUE, PO BOX 280908, HARRISBURG, PA 17128-0908.
For additional information visit www.revenue.state.pa.us or call (717) 783-6277 (electronic filing calls only). Services for taxpayers with
special hearing and/or speaking needs: 1-800-447-3020 (TT only).
B-14](https://image.slidesharecdn.com/stambaughnesspayrollmanual20092010-12629627631222-phpapp01/85/Stambaugh-Ness-Payroll-Manual-2009-2010-43-320.jpg)
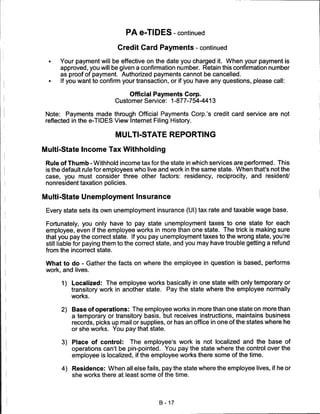





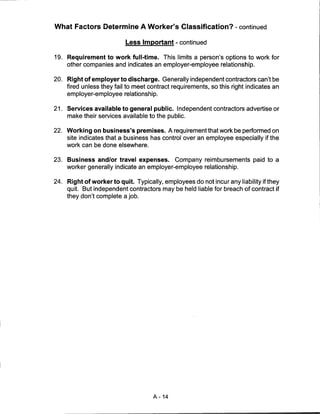
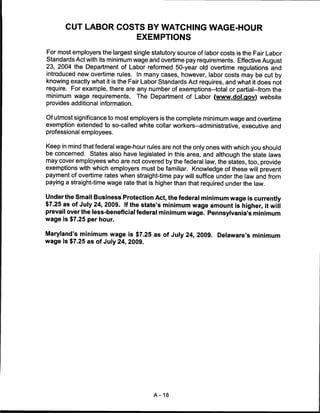
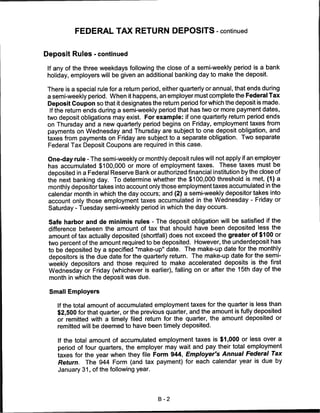
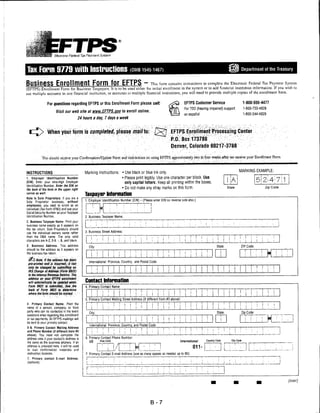
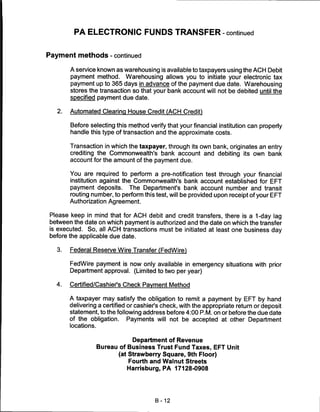
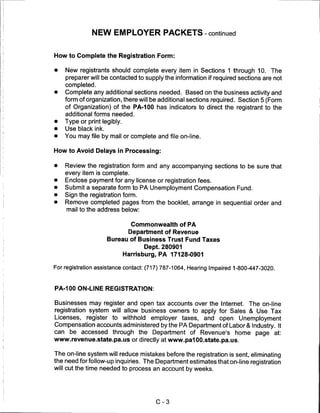
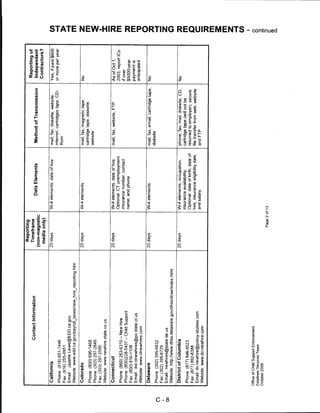
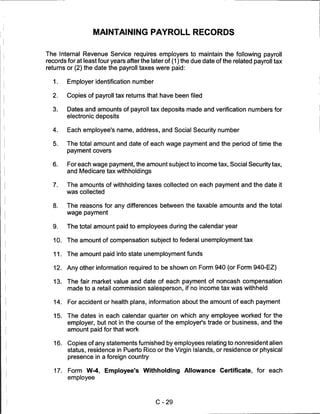
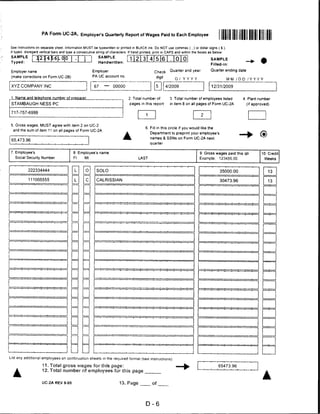
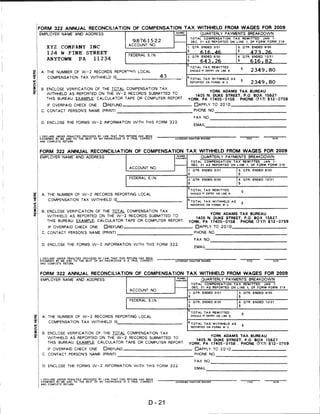
![FORM 1099-MISC
CORRECTED (if checked)
PAYER'S name, street address, city, state, ZIP code, and telephone no. 1 Rents | OMB No. 1545-0115
Miscellaneous
2 Royalties I(Q)09 Income
Form 1099-MISC
3 Other income 4 Federal income lax withheld Copy B
For Recipient
$ £
PAYER'S federal identification RECIPIENT'S identification 5 Fishing boat proceeds 6 Medical and health care payments
number number
$ $
RECIPIENT'S name 7 Nonemployee compensation 8 Substitute payments in lieu of
dividends or interest This is important tax
information and is
being furnished to
the Internal Revenue
$ $ Service. If you are
Street address (including apt. no.) 9 Payer made direct sales of 10 Crop insurance proceeds required to file a
$5,000 or more of consumer return, a negligence
product to a biyer penalty or other
(recip ent) for re ale ► [ ] $ sanction may be
City, state, and ZIP code 11 imposed on you if
this income is
taxable and the IRS
Account number (see instructions) 13 Exce golde i parachute 14 Gro proceeds paid to determines that it
payments an attorney has not been
reported.
$
15a Section 409A deferrals 15b Section 409A income 16 State tax withheld 17 State/Payer's state no. 18 State income
$ $
Form 1099-MISC (keep for your records) Department of the Treasury - Internal Revenue Service
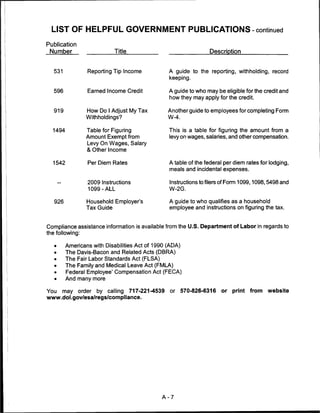
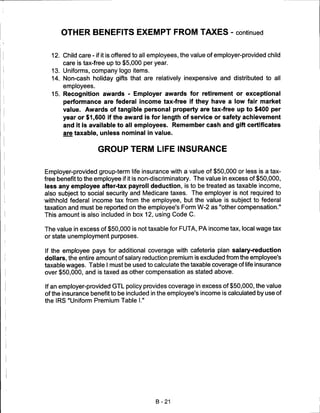
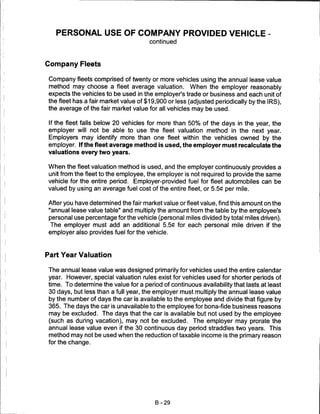
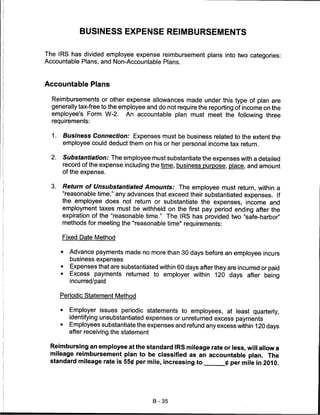
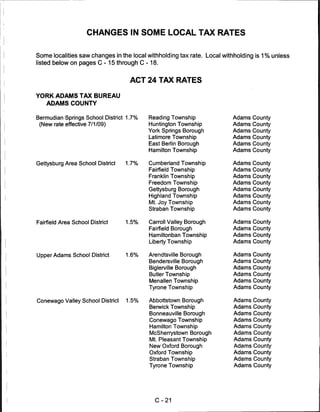
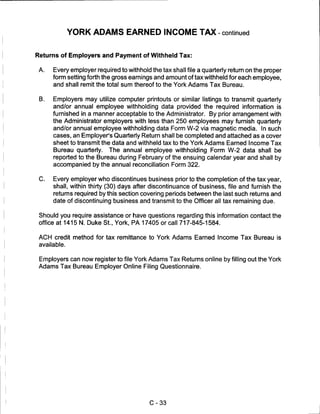
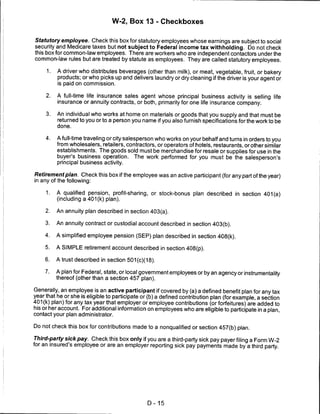
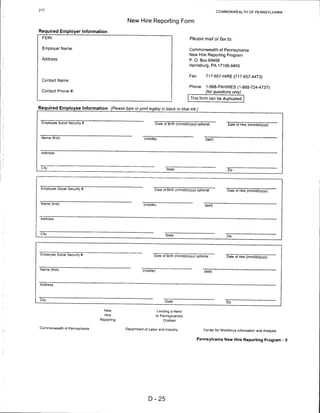
Form 1099-MISC is due to the recipient on February 1 and to the IRS on March 1.
When Forms 1099 are transmitted to the IRS, they must be summarized on Form 1096,
Annual Summary and Transmittal of U. S. Information Returns. A separate Form 1096
should be used for each type of information return submitted to the IRS. Boxes are
provided on the form to indicate the types of information return being submitted.
B-34](https://image.slidesharecdn.com/stambaughnesspayrollmanual20092010-12629627631222-phpapp01/85/Stambaugh-Ness-Payroll-Manual-2009-2010-63-320.jpg)





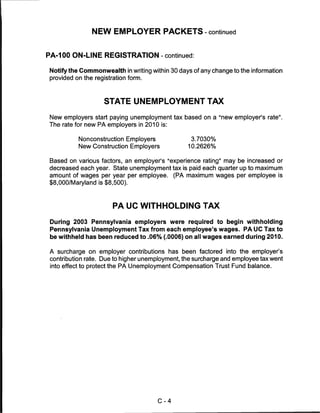


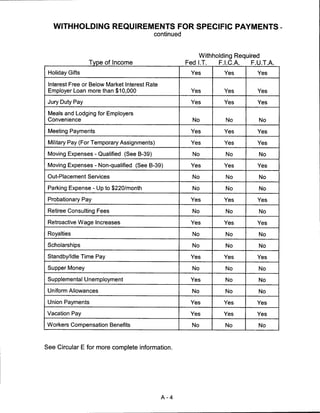
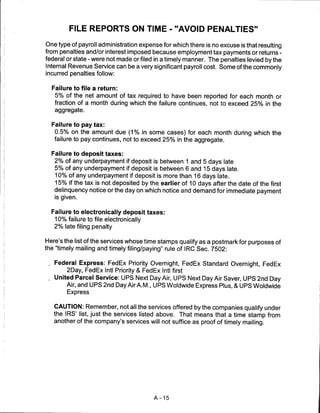
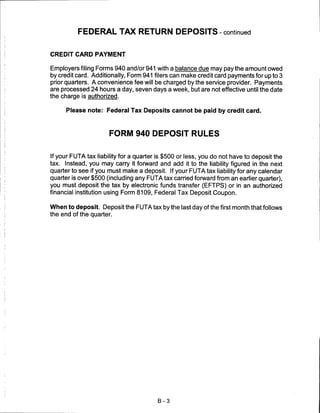
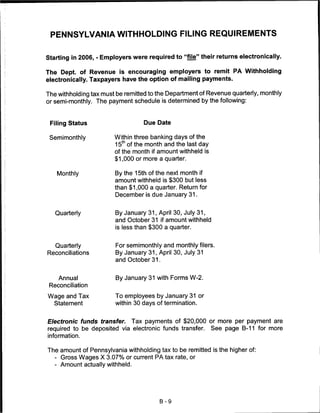
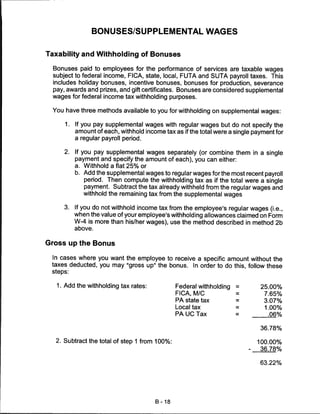
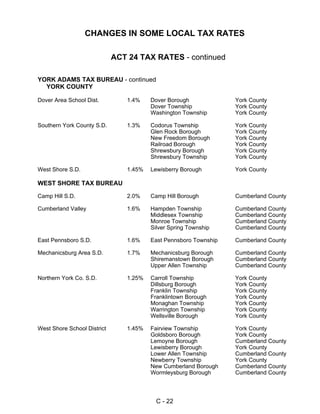
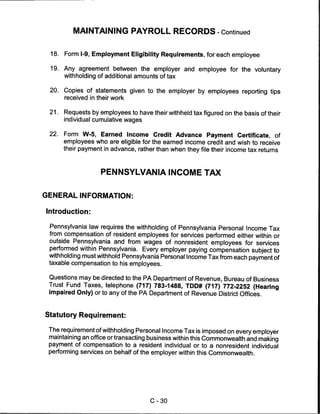
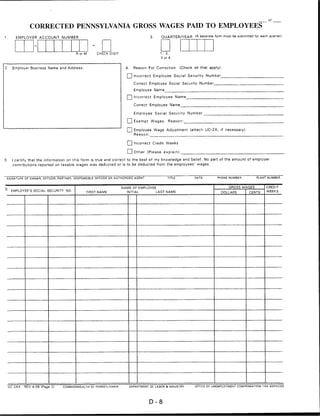
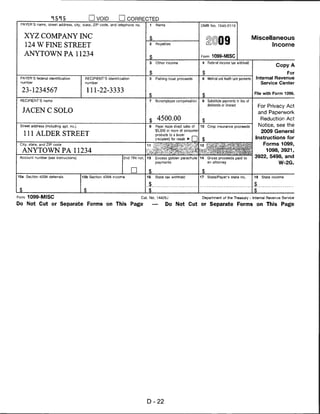
![Reporting
Reporting of
Contact Information Timeframe
Data Elements Method of Transmission Independent
(non-magnetic
Contractors?
media only)
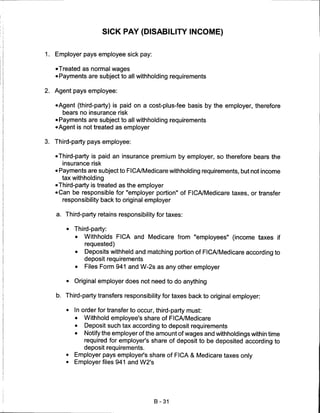
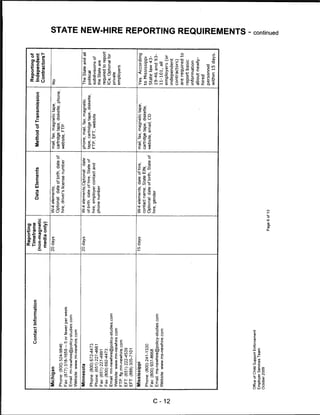
Illinois 20 days W-4 elements; mail, fax, magnetic cartridge & No
Optional: date of hire, address diskette, website and email
Shedrick C. Woods, Manager
for income withholding orders
Phone: (800) 327-HIRE [4473] - Customer Service
Phone: (312) 793-0322 - New Hire
Phone: (312) 793-6298 - Magnetic Media Technical Support
3
m
Fax: (217)557-1947
z
Email: DES.NHire@illinois.gov
Website: wwwides.state.il.us/employer/new-hire.asp
m
Indiana 20 days W-4 elements, date of hire; mail, fax, magnetic tape, No
Optional: date of birth, State of cartridge tape, diskette,
Phone:(866)879-0198
hire; medical insurance website, email, FTP, EFT
Phone:(317)612-3028
Phone: (866) 879-0198, ext. 111 - Technical Support
Fax:(800)408-1388 m
Fax: (317)612-3036
Email: rredmond@policy-studies.com
7)
Website: www.in.gov or www.in-newhire.com
m
"0
Iowa 15 days W-4 elements, date of birth, mail, fax, CD, diskette, Yes*
date of hire, employer's phone, cartridge tape, website
O
Phone: (877) 274-2580 7)
medical insurance availability,
o Fax: (800) 759-5881
I
date of med insurance
Email: csrue@dhs.state.ia.us
qualification, address z
Website: www.iowachildsupport.gov
for income withholding
o
Kansas 20 days W-4 Elements, Fax, mail, CD-Rom, diskette, No
date of hire, FEIN and address website 7)
Phone: (888) 219-7801
for withholding orders m
Phone:(785)296-1716
Fax:(888)219-7798 0
Fax: (785)291-3423 c
Email: newhires@dol.ks.gov
Website, www.dol.ks.gov
m
Kentucky 20 days W-4 elements; Optional: date US mail, fax, magnetic tape, No
of birth, State of hire, date of diskette, website, file upload
Phone:(800)817-2262 m
hire, KY employer ID number, via Internet
Fax: (800)817-0099 z
medical insurance availability,
Email: ky-newhire@policy-studies.com
contact phone
Website: www.kynewhire.com
c
Office of Child Support Enforcement
Employer Services Team
October 2009
Page 4 of 13
CO
Q.](https://image.slidesharecdn.com/stambaughnesspayrollmanual20092010-12629627631222-phpapp01/85/Stambaugh-Ness-Payroll-Manual-2009-2010-80-320.jpg)


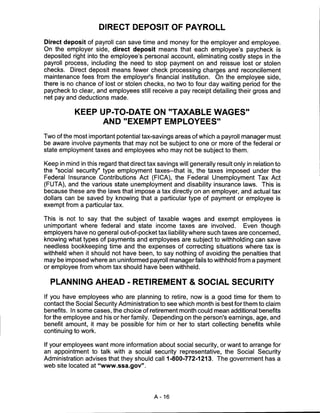
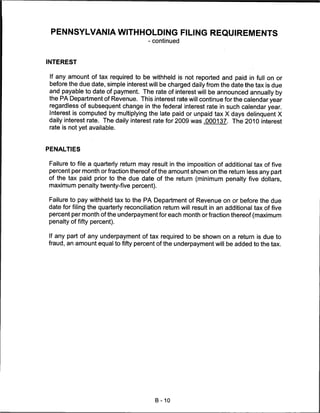
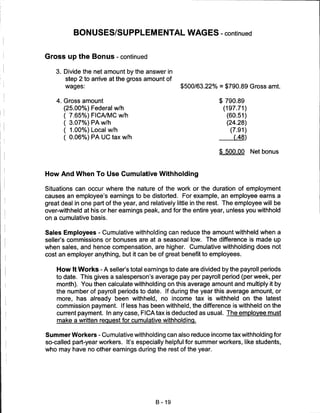
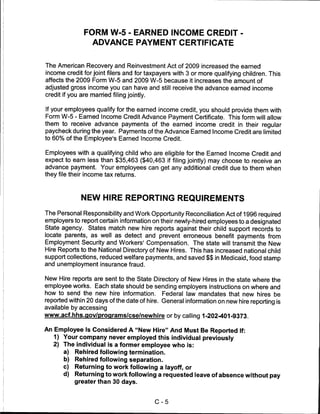
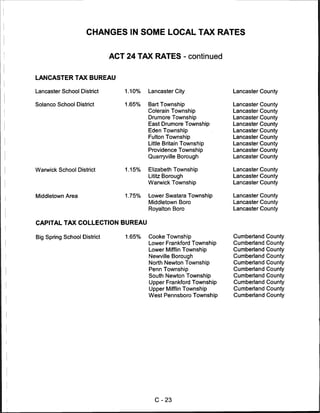
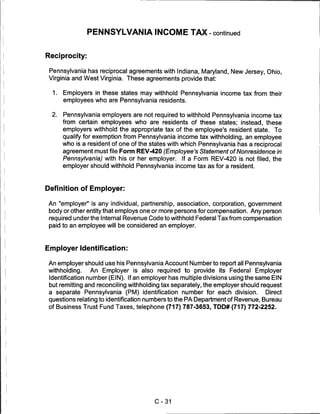
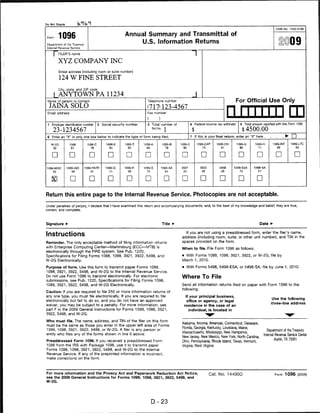
![Reporting
Reporting of
Contact Information Timeframe
Data Elements Method of Transmission Independent
(non-magnetic
Contractors?
media only)
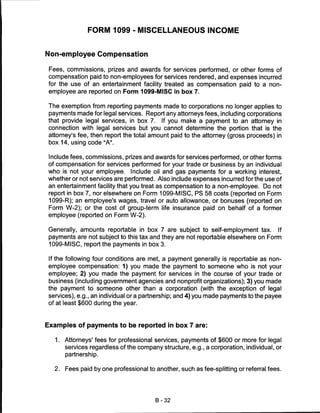
Pennsylvania 20 business days W-4 elements, date of hire, mail, fax, magnetic tape, No CO
employer contact name and diskette, website, email, FTP
Phone: (888) PAHIRES [724-4737]
phone,
Fax: (717) 657-HIRE (4473)
Optional: date of birth
Email: reporting@panewhires.com 3
Website: www.panewhires.com m
ftp:24.104.35.55
z
Puerto Rico 20 days W-4 elements, employer's mail, fax No m
State ID number, date of birth,
Administration for Child Support Enforcement
date of hire, State of hire,
State New Hire Registry
salary
P.O. Box 70376
San Juan, PR 009368376
Phone: (787)767-1500
7)
Fax: (787) 767-3882; 765-1313
m
Rhode Island 14 days W-4 elements, medical phone, mail, fax, magnetic No
insurance availability, date of tape, cartridge tape, diskette, m
Phone: (888) 870-6461 - New Hire
availability; website, Internet upload, FTP
Phone: (401) 222-2847 - Child Support
Optional: date of birth, date of
Phone: (888) 870-6461 - Reporting O
hire, State of hire, payroll
Fax: (888) 430-6907
address
Email: contact@rinewhire.com (info only)
Website: www.Rinewhire.com
FTP: FTP.Rlnewhire.com
South Carolina 20 days W-4 elements;
o
mail, fax, internet upload, No
Optional: date of birth, date of website, FTP 7)
Phone: (888) 454-5294 - New Hire
hire, employer's phone number m
Phone: (803) 898-9235 - New Hire
Phone: (800) 768-5858 - Child Support 0
Fax: (803)898-9100
Website: www.scnewhire.com
73
South Dakota 20 days W-4 elements; phone, mail, fax, cartridge No
m
Optional: date of birth, date of tape, diskette, website
Phone: (888) 827-6078
hire, State of hire
Phone: (605) 626-2942
m
Fax: (888) 835-8659
Fax: (605) 626-2842
z
Website: www.sdjobs.org
CO
Office of Child Support Enforcement
Employer Services Team
§
October 2009
Page 10 of 13 C
CD
Q.](https://image.slidesharecdn.com/stambaughnesspayrollmanual20092010-12629627631222-phpapp01/85/Stambaugh-Ness-Payroll-Manual-2009-2010-86-320.jpg)









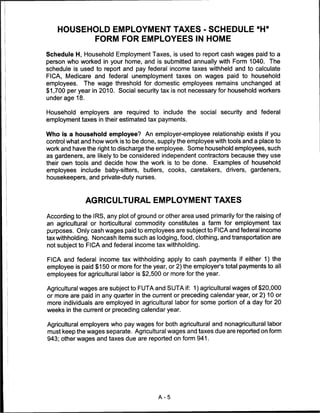
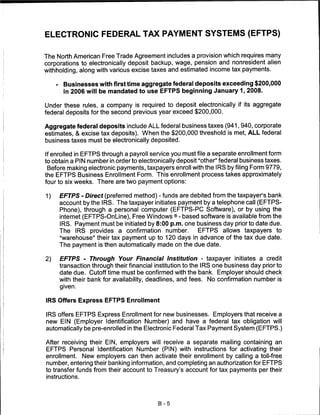
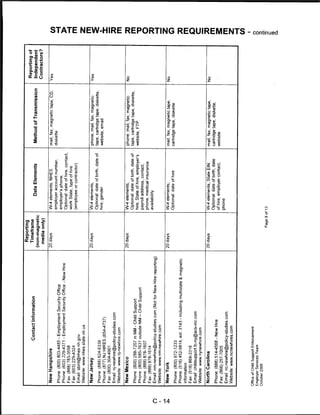
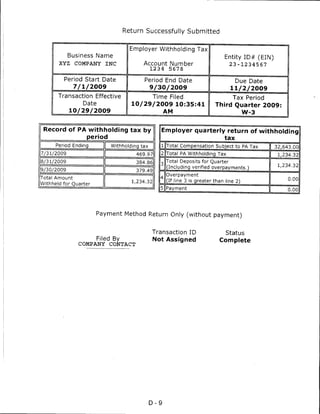
![TRANSMITTAL #
Of
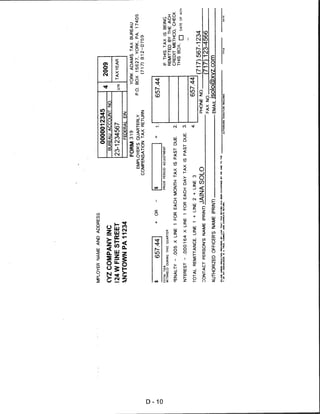
PENNSYLVANIA UNEMPLOYMENT COMPENSATION CORRECTION REPORT
(To Amend Quarterly UC-2/2ATax Reports) (A separate form must be submitted for each quarter)
1. EMPLOYER ACCOUNT NUMBER 3. QUARTER/YEAR
R or M CHECK DIGIT 1, 2,
3 or 4
4. Reason For Adjustment (Check all that apply):
2. Employer Name and Address: Q Incorrect Gross Wages. 'Please explain. Q Exempt Wages Reported in Error.* Please explain:
I I Incorrect Employee Withholding Rate Used LJ Calculation Error. Please explain:
List Rate Used
I I Incorrect Taxable Wages. Please explain: I I Other Error, Please i
□ Incorrect Employer Contribution Rate Used *PR0VIDE 'DIVIDUAL EMPLOYEE CORRECTION
FORM (UC-2AX), IF NECESSARY.
List Rate Used
d Wages Reported to Wrong State • □ PLEASE CHECK IF EMPLOYEE WAGE DETAIL WAS
CORRECTED ON ELECTRONIC MEDIA.
5. Was the employee withholding correctly withheld? Q Yes Q No [J Not applicable (Please see instructions on reverse side.)
AMOUNT PREVIOUSLY
TAX RATE :.'.'■■■:-:' -Vv ■■- ' .-. ^■-":':-, REPORTED CORRECT AMOUNT DIFFERENCE (OVER) UNDER
GROSS WAGES
7. EMPLOYEE WITHHOLDING
B
w *
'■-■'■--■ ' ■■■■.■•:"■ ;-■■.■■: ■•■ . ■;
-..;■.
■■-- ' .
■. ,■ ■{ TAXABLE WAGES
9. EMPLOYER CONTRIBUTION
10.TOTAL (REFUND/CREDIT) OR TAX DUE (ADD LINES 7 AND 9) IN THE DIFFERENCE COLUMN refunos/credits should
BE IN PARENTHESES 1 )
11. Please check one: £~J Refund [~] Credit Q] Not Applicable (Please see instructions on reverse side.)
12. Employer Certification: I certify that the information on this form is true and correct to the best of my knowledge and belief. No part of the
amount of employer contributions reported on taxable wages was deducted or is to be deducted from the employees' wages.
SIGNATURE OF OWNER, OFFICER, PARTNER, RESPONSIBLE OFFICER OR AUTHORIZED AGENT PHONE NUMBER
department use only (do not write below this line) —■
correction report □ journal voucher
SY MO YR QTR YR BASIC CONTRIBUTION INTEREST PENALTY A
(X) WAGES
RATE DEBIT CREDIT DEBIT CREDIT DEBIT CREDIT 4
_J
J
u
u
u
Totals
COMMENTS TOTAL REMITTANCE
Rate Verification Certification: Date Contribution Received Date Report Received
B.I. Audit Needed □ Yes □ No □ N/A Benefit Charges □ Yes □ No □ N/A FSD CERTIFICATION/DATE
TAX TECHNICIAN DATE OTHER REQUIRED SIGNATURE
Vear I ] No Change Rate Revised From Year Q No Change Rate Revised From
UC-2X REV 4-06 (Page 1) COMMONWEALTH OF PENNSYLVANIA DEPARTMENT OF LABOR & INDUSTRY OFFICE OF UC TAX SERVICES
D-7](https://image.slidesharecdn.com/stambaughnesspayrollmanual20092010-12629627631222-phpapp01/85/Stambaugh-Ness-Payroll-Manual-2009-2010-113-320.jpg)
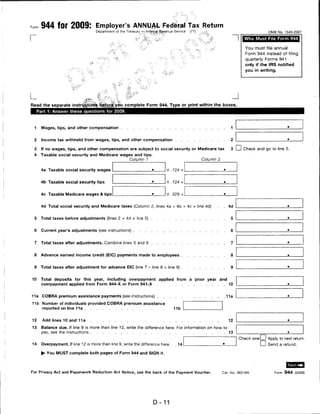
![Form 940 for 2009: Employer's Annual Federal Unemployment (FUTA) Tax Return
Department of the Treasury — Internal Revenue Service OMB No. 1545-0028
(EIN)
f Return
Employer identification number
'" that apply.)
^ame (not your trade name) _
"I 4 a. Amended
Trarte namp (ii any) I I b. SuccessOrtemployer
. ■ ■..r;' ,■:; ■■ -T-.
I I • ;c. Np.payments to employees
Address
Number Street ... Suite or room number v^.:;- y:-..'i -.V,~
, d;.;EinaJ|:Business closed or
vfc ped paying wages
City .•■■•State ZIP code
Read the separate instructions before youifjiKout this form. Please type or priqtjwittiiri tfie boMsyii'*
1 If you were required to pay your state unpfrtployrnent tax iti ..-."> .'•^ *"h v
1a One state only, write the state abbreviation . "■?."". 4. 1a1
- OR - ;C: %v %.
1 b More than one state (You are a multi-statejsempjbyer)>l.-ti 1b CD Check here. Fill out Schedule A.
2 If you paid wages in a state that is subject to CREDIT REDUCTION 2 I I Check here. Fill out Schedule A
(Form 940), Part 2.
Part 2: Determine your FUTA tax before adjustments for 2009. If any line does NOT apply, leave it blank.
3 Total payments to all employees
4 Payments exempt from FUTA tax 4
Check all that apply: 4a LJ Fringe benefits 4c I I Retirement/Pension 4e I I Other
4b I ] Group-term life insurance 4d I I Dependent care
5 Total of payments made to each employee in excess of
$7,000 5
6 Subtotal (line 4 + line 5 = line 6) 6
7 Total taxable FUTA wages (line 3 - line 6 = line 7) 7
8 FUTA tax before adjustments (line 7 x .008 = line 8) 8
Part 3: Determine your adjustments. If any line does NOT apply, leave it blank.
9 If ALL of the taxable FUTA wages you paid were excluded from state unemployment tax,
multiply line 7 by .054 (line 7 X .054 = line 9). Then go to line 12 9
10 If SOME of the taxable FUTA wages you paid were excluded from state unemployment tax,
OR you paid ANY state unemployment tax late (after the due date for filing Form 940), fill out
the worksheet in the instructions. Enter the amount from line 7 of the worksheet 10
11 If credit reduction applies, enter the amount from line 3 of Schedule A (Form 940) . . 11
Part 4: Determine your FUTA tax and balance due or overpayment for 2009. If any line does NOT apply, leave it blank.
12 Total FUTA tax after adjustments (lines 8 + 9 + 10 + 11 = line 12) . . 12
13 FUTA tax deposited for the year, including any overpayment applied from a prior year . .13
14 Balance due (If line 12 is more than line 13, enter the difference on line 14.)
• If line 14 is more than $500, you must deposit your tax.
• If line 14 is $500 or less, you may pay with this return. For more information on how to pay, see
the separate instructions 14
15 Overpayment (If line 13 is more than line 12, enter the difference on line 15 and check a box
below.) . 15
Check one: Lj Apply to next return.
► You MUST fill out both pages of this form and SIGN it. I I Send a refund.
For Privacy Act and Paperwork Reduction Act Notice, see the back of Form 940-V, Payment Voucher. Cat. No. 11234O Form 940 (2009)
D-17](https://image.slidesharecdn.com/stambaughnesspayrollmanual20092010-12629627631222-phpapp01/85/Stambaugh-Ness-Payroll-Manual-2009-2010-123-320.jpg)



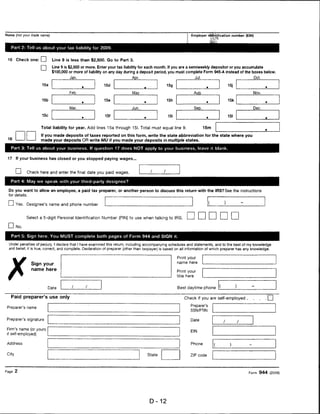
![DO NOT CUT, FOLD, OR STAPLE THIS FORM
For Official Use Only ►
M "4 4 M M
OMB No, 1545-0008
a Employer's ne me. address, and ZIP code c Tax year/r-orm corrected d Employees correct SSN
XYZ COMPANY INC 222-33-7777
2 0 0 9 / W-2
124 W FINE STREET
e Corrected SSN and/oi name (Check this box and complete boxes f and/or
ANYT OWN PA 112 34 g if incorrect on form previously filed.) r~i
Complete boxes f and/or g only it incorrect on form previously filed ►
f Employee's previously reported SSN
b Employer's Federal EIN g Employee's previously reported name
23-1234567
h Emplo yee's first name and initial Last name Sufi
JA]:na SOLO
777 SKY LANE
Note: Only complete money fields that are being corrected
(exception: for corrections involving MQGE, see the Instructions ANY TOWN PA 11234
for Forms W-2c and W-3c, boxes 5 and 6). i Emplo yee's address and ZIP code
Previously reported Correct information Previously reported Correct information
1 Wages, tips, other compensation 1 Wages, tips, other compensation 2 Federal income tax withheld 2 Federal income tax withheld
92400.00 95000.00 12574 .00 23750.00 .
3 Social security wages 3 Social security wages 4 Social security tax withheld 4 Social security tax withheld
92400.00 95000.00 5728.80 5890.00
5 Medicare wages and tips 5 Medicare wages and tips 6 Medicare tax withheld 6 Medicare tax withheld
92400. 00 95000.00 _j 1339.80 1377.50
7 Social security tips 7 Social security tips 8 Allocated tips 8 Allocated tips
9 Advance EIC payment 9 Advance EIC payment 10 Dependent care benefits 10 Dependent care benefits
11 Nonqualified plans 11 Nonqualified plans 12a See I istructions for box 12 12a See instructions for box 12
o
d
13 Statutory Kellrpineiu Tlrint-partv 13 Statutory Retirement 1 hint-party
prnploveii plan sitt. nav ampUiyee plan skk nay
12b 12b
c
□ □ n □ n it 3
14 Other (see inst ructions) 14 Other (sse instructions) 12c 12c
t:
? ,., .
12d 12d
Stale Correction Information
Previously reported Correct information . Previously reported Correct information
15 State 15 State 15 State 15 State
PA PA
Employer s state ID number Employer's state ID number Employer's state ID number Employer's state ID number
1234 5678 1234 5678
16 State wages, tips, etc. 16 State wages, tips. etc. 16 State wages, tips, etc. 16 State wages, tips. etc.
92400.00 95000.00
17 State income tax 17 State income tax 17 State income lax 17 State income lax
2574.20 2916.50
Locality Correction information
Previously reported Correct information Previously reported Correct information
18 Local wages, tips, etc. 18 Local wages, tips, etc. ^ - Vaf* to6aVwages, tips, etc. 18 Local wages, tips, etc.
92400.00 95000.00
19 Local income tax 19 Local income tax 19 Local income tax 19 Local income tax
838.50 950.00
20 Locality name 20 Locality name 20 Locality name 20 Locality name
ANYTOWN ANYTOWN
For Privacy Act and Paperwork Reduction Act Notice, see separate instructions. Copy A—For Social Security Administration
Form W-2C (Rev. 2-2009) Corrected Wage and Tax Statement Department of the Treasury
Cat. No. 61437D Internal Revenue Service
D-30](https://image.slidesharecdn.com/stambaughnesspayrollmanual20092010-12629627631222-phpapp01/85/Stambaugh-Ness-Payroll-Manual-2009-2010-136-320.jpg)





This document provides a guide to payroll and payroll tax information for 2009-2010. It includes charts with tax rates, wage limits, and taxability of compensation. It also offers tips to save on payroll such as using independent contractors, direct deposit, retirement planning, and available tax credits. Contact information is provided for Juanita Aubel, the tax advisor, along with tables of contents listing the guide's parts on processing and reporting, startup information for new employers, and specific payroll forms.




































