Presentation given by Dr Adnan Saithna, Professor of Orthopedic Surgery at AAOS 2020, on factors influencing outcomes of a validated return to sports test battery after ACL reconstruction
Deborah Stein SMACC Chicago talk Trauma is Risky Business - delves into the risk patients and physicians undergo when treating or being treated for Trauma.
Stein’s speaks of the Risk Benefit Determination that physicians make daily and how this is used to best answer on going questions such as; can a patient have?, how do we care for this patient? and how do we best make all the these decisions?. Stein’s suggests a thorough Risk Benefit Determination will include:
Analysis of best available data
Use of best available judgement
Gathering of different opinions
An understanding that you won’t always make the right decision
To document the 'crap' out of it!
And to remember you’ll never know what you prevented from not occurring.
Stein’s also focuses on the risk to patients due to missed injuries and the processes physicians can take to help ensure that a patient injuries are not missed. Stating that 1.3-39% of injuries in trauma are missed (a majority of which present as orthopaedic cases).
Touching on the processes designed to prevent missed injuries such as;
Territory Trauma Survey
Roles of clinical decision rules
To scan the living ‘crap’ out of them - whole body CT scans (can decrease mortality but comes attached with its own risks).
Stein’s then delves into the risks trauma providers (physicians) face on a daily bases. Stating that in the USA trauma providers are one of the highest categories of physicians to be sued, have higher indemnity payment awarded against them and achieve a higher risk score in studies for being sued. While, lawsuits are more likely to increase the chance of physician burnout, career burnout, depression and are emotionally and physically exhausting. Steins sights recent studies that suggest the more open, honest and forthright a physician is with their error with their peers and their hospital the likelihood of being sued reduces.
Stein’s also notes that needle stick injuries in most departments have decreased in recent years due to universal precautions, yet have increased in trauma care due to the nature of the ER environment and proper precautions not being taken. Violence is of risk to attending ER nurses, physicians and paramedics, sighting an Australian study that 79% of triage nurses have experienced physical violence from patients. And, the emotional harm the trauma environment can have on trauma providers.
Steins suggests that trauma providers must be aware and learn how to manage risk better to ensure patient and provider safety.
Bo Abrahamsen's presentation from Osteoporosis 2016: Surgically treated osteonecrosis and osteomyelitis of the jaw and oral cavity in patients highly adherent to alendronate treatment.
Find out more at: https://nos.org.uk/conference
Case-control Study on 2nd Hammertoe Deformity Correction TechniquesWenjay Sung
This is my case-control study on second hammertoe deformity correction techniques: arthroplasty, arthrodesis, and interpositional implant arthroplasty.
Presentation given by Dr Adnan Saithna, Professor of Orthopedic Surgery at AAOS 2020, on factors influencing outcomes of a validated return to sports test battery after ACL reconstruction
Deborah Stein SMACC Chicago talk Trauma is Risky Business - delves into the risk patients and physicians undergo when treating or being treated for Trauma.
Stein’s speaks of the Risk Benefit Determination that physicians make daily and how this is used to best answer on going questions such as; can a patient have?, how do we care for this patient? and how do we best make all the these decisions?. Stein’s suggests a thorough Risk Benefit Determination will include:
Analysis of best available data
Use of best available judgement
Gathering of different opinions
An understanding that you won’t always make the right decision
To document the 'crap' out of it!
And to remember you’ll never know what you prevented from not occurring.
Stein’s also focuses on the risk to patients due to missed injuries and the processes physicians can take to help ensure that a patient injuries are not missed. Stating that 1.3-39% of injuries in trauma are missed (a majority of which present as orthopaedic cases).
Touching on the processes designed to prevent missed injuries such as;
Territory Trauma Survey
Roles of clinical decision rules
To scan the living ‘crap’ out of them - whole body CT scans (can decrease mortality but comes attached with its own risks).
Stein’s then delves into the risks trauma providers (physicians) face on a daily bases. Stating that in the USA trauma providers are one of the highest categories of physicians to be sued, have higher indemnity payment awarded against them and achieve a higher risk score in studies for being sued. While, lawsuits are more likely to increase the chance of physician burnout, career burnout, depression and are emotionally and physically exhausting. Steins sights recent studies that suggest the more open, honest and forthright a physician is with their error with their peers and their hospital the likelihood of being sued reduces.
Stein’s also notes that needle stick injuries in most departments have decreased in recent years due to universal precautions, yet have increased in trauma care due to the nature of the ER environment and proper precautions not being taken. Violence is of risk to attending ER nurses, physicians and paramedics, sighting an Australian study that 79% of triage nurses have experienced physical violence from patients. And, the emotional harm the trauma environment can have on trauma providers.
Steins suggests that trauma providers must be aware and learn how to manage risk better to ensure patient and provider safety.
Bo Abrahamsen's presentation from Osteoporosis 2016: Surgically treated osteonecrosis and osteomyelitis of the jaw and oral cavity in patients highly adherent to alendronate treatment.
Find out more at: https://nos.org.uk/conference
Case-control Study on 2nd Hammertoe Deformity Correction TechniquesWenjay Sung
This is my case-control study on second hammertoe deformity correction techniques: arthroplasty, arthrodesis, and interpositional implant arthroplasty.
Imogen Mitchell - Morphing the Recalcitrant ClinicianSMACC Conference
Imogen Mitchell’s SMACC Chicago talk 'Morphing the Recalcitrant Clinician’ talks us through the steps to engage the reluctant physician when implementing change.
Imogen initally touches on the stages of physician engagement from aversion, to apathy, to engaged and then outlines the steps to morphing the reluctant physician.
1. Seek out a clinical champion
2. Establish a common purpose/vision
3. Standardise what is standardisable
4. Communication, communication, communication
5. Work out barriers and overcome them
6. Deal with the ‘Whats in it for me?’WIFM
Physical Therapy in the Emergency Departmentchristaloyd
At the Heart of the Rockies Regional Medical Center in Salida, CO, I got the opportunity to take the lead on doing research and analyzing data to create a presentation describing the benefits of Physical Therapy in an emergency department.
Imogen Mitchell - Morphing the Recalcitrant ClinicianSMACC Conference
Imogen Mitchell’s SMACC Chicago talk 'Morphing the Recalcitrant Clinician’ talks us through the steps to engage the reluctant physician when implementing change.
Imogen initally touches on the stages of physician engagement from aversion, to apathy, to engaged and then outlines the steps to morphing the reluctant physician.
1. Seek out a clinical champion
2. Establish a common purpose/vision
3. Standardise what is standardisable
4. Communication, communication, communication
5. Work out barriers and overcome them
6. Deal with the ‘Whats in it for me?’WIFM
Physical Therapy in the Emergency Departmentchristaloyd
At the Heart of the Rockies Regional Medical Center in Salida, CO, I got the opportunity to take the lead on doing research and analyzing data to create a presentation describing the benefits of Physical Therapy in an emergency department.
To Determine Preference of Shoulder Pain Management by General Physicians in ...suppubs1pubs1
Rotator cuff muscles are functionally active and provide stability to the shoulder joint and also thereby allow the full Range of Motion (ROM) by moving the head of humerus in the glenoid cavity. Any tear or fragility of the rotator cuff muscles can cause the dislocation or instability and hence damaging other muscles specially the long head of biceps muscle. The diseases related to the supraspinatus tendon are frequently linked with the long head of the biceps tendon. Other cause of chronic shoulder pain is the adhesive capsulitis with large prevalence rates of more than 5.3% in the general target population [3].
Abstract
Background: Physiotherapy is multi-dimensional and can treat a vast variety of conditions, ranging from musculoskeletal aches, arthritis, joints problems, paraplegia, hemiplegic, sports injuries and frozen shoulder etc. Apart from culture competency and core medical knowledge a physiotherapist must be competent enough in all physiotherapist medical conditions where physical therapy plays a vital role. This study aims to identify the frequency of common clinical conditions among client presented at Habib Physiotherapy Complex (HPC), Hayatabad during 2010.
Methodology: This was a descriptive study; the data were retrieved from record register of HPC (Indoor and Outdoor patients) recording their presenting complaints and known diagnoses. Data was collected on a structure grid. Data was analyzed using SPSS version 15 and presented in term of frequency and percentages.
Result: The majority of clients (1280 (29%)) were suffering from low back pain. The second common condition 891(20%) was osteoarthritis of the knee joint and cerebrovascular accidents 824(18.4%), while cervical pain accounted for 734(16.4%). The rest of clinical conditions included; frozen shoulder, pelvic inflammation, cerebral palsy, polio effected and paraplegia.
Conclusion: The Study reveals the occurrence of Osteoarthritis (Low Back, Cervical Pain, and Knee Joints Pain) were the most common condition which deteriorated the performance of common individuals in our society.
Austin Journal of Musculoskeletal Disorders is a peer-reviewed, open access journal published by Austin Publishers. It provides easy access to high quality Manuscripts in all related aspects of diseases and disorders that may adversely affect the function and overall effectiveness of the musculoskeletal system. The Journal focuses upon all the related aspects of musculoskeletal system disorders and the new advancements in the related treatments including Complex issues and injuries involving the musculoskeletal system and surgeries.
Austin Publishing Group is a successful host of more than hundred peer reviewed, open access journals in various fields of science and technology with intent to bridge the gap between academia and research access.
Austin Journal of Musculoskeletal Disorders accepts original research articles, review articles, case reports, mini reviews, rapid communication, opinions and editorials on all related aspects of diseases and disorders that may adversely affect the function and overall effectiveness of the musculoskeletal system.
1. Inpatient Versus Outpatient Outcomes in Total Hip Arthroplasty Patients
Peggy Essick, MS, CCRP; Tamiko MaGee, MS, CCRP: Noah Sheeley, BS
Introduction
Osteoarthritis, the most common form of joint disease and
affecting millions of people, is regarded as a major cause of
disability, psychological distress, and poor quality of life1.
Joint replacement surgery may be indicated when a person
has severe symptoms and no longer responds to
conservative management. Total hip arthroplasty (THA) is
a commonly performed surgical procedure that helps to
reduce pain and improves both joint function and quality of
life. According to the Centers for Disease and Control and
Prevention, over 330,000 total hip replacements are
performed each year. Healthcare reform has prompted
health care systems to reduce costs, which includes shorter
hospitalization stays. Although, total knee arthroplasty
(TKA) performed on an outpatient basis has become fairly
common, outpatient THA is much less common. Healthcare
providers are beginning to include outpatient THA as a
feasible option for some patients.
Our goal for this poster was to determine if the length of
hospitalization following a THA would have any effect
on self-reported or functional outcomes.
References
1.Barnsley, Lara, Leslie Barnsley, and Richard Page. "Are Hip
Precautions Necessary Post Total Hip Arthroplasty? A
Systematic Review." Geriatric Orthopaedic Surgery &
Rehabilitation (2015): 2151458515584640.
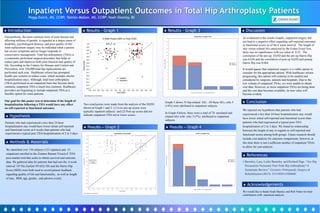
Results - Graph 1 Results – Graph 3
Methods & Materials
We identified over 158 subjects (123 inpatient and 35
outpatient) enrolled in the Zimmer Biomet Vivacit-E THA
post-market trial that seeks to obtain survival and outcome
data. We gathered data for patients that had met the 6 week
interval. Of The EurQol 5D (EQ 5D) and the Harris Hip
Score (HHS) were both used to record patient feedback
regarding quality of life and functionality, as well as length
of stay, BMI, age, gender, and adverse events.
Hypothesis
Patients who had experienced a less than 24-hour
hospitalization stay would have lower initial self-reported
and functional scores at 6 weeks than patients who had
experienced a typical post THA hospitalization of 2 to 3 days
Discussion
As evidenced in the results Graphs, outpatient surgery did
not lead to a negative effect regarding self-reported outcomes
or functional scores as of the 6 week interval. The length of
stay versus related AEs analyzed by the Fisher Exact Test,
there was no significance with a p-value of 0.22. The
correlation of the pre-op EQ5D and the pre-op Harris Hip
was 0.626 and the correlation of post op EQ5D and postop
Harris Hip was 0.684.
It would appear that outpatient surgery is a viable option to
consider for the appropriate patient. With healthcare reform
progressing, this option will continue to be studied and
considered by surgeons, patients and hospitals. Due to the
low volume of outpatient THAs, we were unable to obtain
cost data. However, as more outpatient THAs are being done
and the cost data becomes available, its true value will
become evident.
Conclusion
We rejected our hypothesis that patients who had
experienced a less than 24 hour hospitalization stay would
have lower initial self-reported and functional scores than
patients who had experienced a typical post-THA
hospitalization of 2 to 3 days. We found no relationship
between the length of stay in regards to self-reported and
functional scores among both groups. Future research should
include cost analysis for outcome comparisons; however, at
this time there is not a sufficient number of outpatient THAs
to allow for cost analysis.
Acknowledgements
We would like to thank Noah Sheeley and Rob Neher for their
contribution with statistical analysis.
Results – Graph 2
Two conclusions were made from the analysis of the EQ5D
shown in Graph 1 and 2: (1) Low pre-op scores were
typically inpatient subjects and (2) Post-op scores did not
indicate outpatient THA led to lower scores.
Graph 3 shows 35 hip-related AEs . Of these AEs, only 5
(14%) were attributed to outpatient subjects.
In Graph 4 below, there were a total of 70 unrelated and
related AEs with only 5 (7%) attributed to outpatient
subjects.
Results – Graph 4