The document describes a quality improvement project to increase efficiency for last cases scheduled in a busy PET-CT center. A multi-disciplinary team used lean sigma principles to assess the problem and identify solutions. Data was collected from September 2014 to April 2015 on last case completion times. Interventions like starting the first case earlier, changing patient scheduling and staff schedules helped increase on-time completion of last cases from 47% to 91% while reducing overtime. The percentage of cases finishing after 6 PM was eliminated.
When a patient registers at a GP practice, GP2GP will be used to electronically transfer their Electronic Health Record (EHR) from their previous GP practice. GP2GP electronic transfers are faster, more reliable and more secure than the current paper-based method of transferring patient records. GP2GP is not a replacement for the transfer of paper-based records, which must continue for the foreseeable future until 100% of GP practices are GP2GP enabled.
When a patient registers at a GP practice, GP2GP will be used to electronically transfer their Electronic Health Record (EHR) from their previous GP practice. GP2GP electronic transfers are faster, more reliable and more secure than the current paper-based method of transferring patient records. GP2GP is not a replacement for the transfer of paper-based records, which must continue for the foreseeable future until 100% of GP practices are GP2GP enabled.
This was a presentation done in a symposium on tele-psychiatry at Annual Conference of Indian Psychiatric Society South Zone, held at Chennai on 15 October 2016
A FEASIBILITY STUDY OF REMOTE MONITORING OF CAPD PATIENT’S BLOOD PRESSURE AND
BLOOD GLUCOSE MEASUREMENTS VIA THE INTERNET. G. Pylypchuk, P. Jacobson, C. McAllister
University of Saskatchewan, St. Paul’s Hospital, Saskatoon, Saskatchewan. Regina, Saskatchewan
The purpose of this study was to determine the feasibility of remotely monitoring blood pressure (BP) and
glucose measurements in a cohort of diabetic patients receiving continuous ambulatory peritoneal
dialysis (CAPD).
The patient handoff is a contemporaneous, interactive process of passing patient-specific information from one caregiver to another to ensure the continuity and safety of patient care. It is well recognized that the handoff is a point of vulnerability where valuable patient information can be distorted and omitted [1, 2]. A plethora of studies in the nursing literature have identified a variety of problems, including incomplete or inaccurate information [3-6], uneven quality [7], repeated interruptions and lack of anticipatory guidance [8]. Many reports have focused on characterizing the weaknesses with non-operative patient handovers, the use of handoff checklists and aviation safety models for specific groups of patients [1,5,9], and the pre- and post-implementation comparisons. [10-12] However, few studies have focused on prospective cohort studies validating and testing patient information management systems such as smart-templates in the setting of handover quality. [10]
Electronic templates containing patient information help to standardize the type of information conveyed during interactions, discourages ambiguous findings,[13] improves provider satisfaction and improves continuity of care.[14] Within the department, we developed the transfer template (T2) to address the issues in provider workflow and efficiency. With the press of a button, the T2 template automatically extracts live information from the anesthetic record, pertinent fields from the PAC note and laboratory values from IView, and provides a concise output of these relevant details.
This was a presentation done in a symposium on tele-psychiatry at Annual Conference of Indian Psychiatric Society South Zone, held at Chennai on 15 October 2016
A FEASIBILITY STUDY OF REMOTE MONITORING OF CAPD PATIENT’S BLOOD PRESSURE AND
BLOOD GLUCOSE MEASUREMENTS VIA THE INTERNET. G. Pylypchuk, P. Jacobson, C. McAllister
University of Saskatchewan, St. Paul’s Hospital, Saskatoon, Saskatchewan. Regina, Saskatchewan
The purpose of this study was to determine the feasibility of remotely monitoring blood pressure (BP) and
glucose measurements in a cohort of diabetic patients receiving continuous ambulatory peritoneal
dialysis (CAPD).
The patient handoff is a contemporaneous, interactive process of passing patient-specific information from one caregiver to another to ensure the continuity and safety of patient care. It is well recognized that the handoff is a point of vulnerability where valuable patient information can be distorted and omitted [1, 2]. A plethora of studies in the nursing literature have identified a variety of problems, including incomplete or inaccurate information [3-6], uneven quality [7], repeated interruptions and lack of anticipatory guidance [8]. Many reports have focused on characterizing the weaknesses with non-operative patient handovers, the use of handoff checklists and aviation safety models for specific groups of patients [1,5,9], and the pre- and post-implementation comparisons. [10-12] However, few studies have focused on prospective cohort studies validating and testing patient information management systems such as smart-templates in the setting of handover quality. [10]
Electronic templates containing patient information help to standardize the type of information conveyed during interactions, discourages ambiguous findings,[13] improves provider satisfaction and improves continuity of care.[14] Within the department, we developed the transfer template (T2) to address the issues in provider workflow and efficiency. With the press of a button, the T2 template automatically extracts live information from the anesthetic record, pertinent fields from the PAC note and laboratory values from IView, and provides a concise output of these relevant details.
Optimising the Model of Care for Patient Management at The Tweed Cancer Care ...Cancer Institute NSW
The commonly understood model of shift to shift nursing handover does not apply to most ambulatory day treatment units. Nonetheless, ‘handover’ of patient clinical information remains quintessential to safe clinical practice. Of considerable interest is how EMR may aid the transfer of patient clinical information in these circumstances and address the question: does this facilitate improved patient care?
This is a study case in all the photosthe SIPOC diagram bel.pdfjkcs20004
This is a study case in all the photos
the SIPOC diagram bellow is incomplete and wrong I need to fix it
Perfect Match TEAM APPLIES n January 2008, the University of Toledo Medical Center
(UTMC) in northwest Ohio collaborated with the University of Toledo's Industrial SIX SIGMA
TO Engineering Department to analyze and improve the preoperational processes for patients
undergoing kidney transplants. Six Sigma was applied to the REDUCE TIME project, and the
following goals were established: IT TAKES TO - Optimize cycle times. QUALIFY PATIENTS
- Enhance customer satisfaction. - Improve efficiencies. FOR KIDNEY - Reduce costs.
TRANSPLANTS - Streamline administrative processes. - Eliminate errors. - Improve protocol
execution and effectiveness. The project's primary metric was the number of days required from
the date a patient was referred to UTMC for a kidney transplant to the date the hospital staff
declared the patient a suitable transplant candidate. The research By Matthew was needed and
the project selected because of an increase in the number of Franchetti and year because of the
increased service area for UTMC. Because of a waiting list of nearly 500 patients, it was
determined a reduced cycle time would save lives. Kyle Bedal, Background and terminology
University of For more than 30 years, UTMC has performed adult and pediatric kidney Toledo
transplants as one of the treatment options for end-stage renal disease. Since UTMC's first
kidney transplant operation in 1972, more than 1,500 kidney transplant operations have been
performed there, with an average patient survival rate of 98% and a graft survival rate of 94%.
The program relies on advanced surgical techniques-including laparoscopic kidney donation,
improved anti-rejection medications and high-quality patient care-to make it one of the most
successful programs in the country. There are a number of steps patients must complete before
receiving a kidney transplant. Generally, the patient must be referred to a medical center and
complete required labs and tests to determine if he or she is suitable. The labs and tests are
usually similar among all transplant centers and among patients. The labs include tuberculosis
(TB) tests, dental clearance, a colonoscopy, chest X-rays, electrocardiography tests, stool
samples, blood work, mammograms, pap smears and diabetes tests. Once the patient fulfills the
requirements, a committee reviews the results and determines whether the patient is a good
candidate. The patient is then allowed to receive a kidney; this is called being "listed," or placed
on the waiting list.
Fil TB EK Often, the time required to complete these health Partnering With Your Transplant
Team, The Patient's Guide screenings is up to nine months. In addition, another to
Transplantation. 2 two years may pass after the patient is listed before a The team deployed the
define, measure, analyze, kidney transplant is performed. improve and control (DMAIC)
approach for this Six It is.
Clinical Data Quality in Mozambique: A Comparative ExerciseJSI
Presentation for the American Public Health Association & Expo in Atlanta, GA. November 2017:
Ensuring that quality data are collected and reported to the Ministry of Health (MOH) is a priority in Mozambique as it is the foundation for the provision of quality health services. Since 2014, the Strategic Information Project in Mozambique (M-SIP) has provided technical assistance to MOH to conduct annual rounds of data quality assessments (DQA) in each province. Seven indicators were selected as part of the national DQA strategy. Each DQA had a quantitative and a system assessment component. The quantitative component includes tracing and verification of reported data, where recounted data is compared to data reported at three levels: health facility (HF), district, and province. M-SIP conducted all DQAs using the same methodology making the results comparable. After three consecutive national rounds, there is a clear trend of improvement, despite deviations remaining high. The regular, reinforcing nature of this activity and consistency of HF recommendations has had a positive impact on the data quality and results of the assessments. For example, the overall national deviation of the “patients active in ART” indicator decreased from 37% to 22% over the three-year period. The successful implementation of the DQA activity, as well as its unique, inclusive approach to promoting MOH ownership, has resulted in MOH recognition—at all levels—that DQA activities are crucial to future success. The M-SIP and MOH teams are now developing a more methodological approach to MOH staff empowerment, enabling fully independent MOH implementation of this activity while continuing to improve the quality of data.
Similar to SNM Abstract poster B.M. Gebrewold (20)
Clinical Data Quality in Mozambique: A Comparative Exercise
SNM Abstract poster B.M. Gebrewold
1. System Improvement to Increase Last Case Efficiency in a busy PET-CT Center
Bineyam Gebrewold1 M.P.H., C.N.M.T. , R.T. (N) (C.T.) , Corina Voicu2 C.N.M.T. , R.T. (C.T.) Esther Mena2 M.D. , Natarsha Fields2 PSC 2, Rathan Subramanian2 M.D., Ph.D.
The Russell H. Morgan Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, Baltimore, MD, U.S.A.
Work flow efficiency is highly impacted by the timeliness of all the
cases through the day in a department like PET-CT that require
longer physiological preparation before a scan can be done. At
Johns Hopkins PET center patient scheduling is handled very
carefully to avoid camera down time between subsequent patients
throughout the day. Any delay between continuous patients will
have a compounding effect on the remaining cases and results in
delayed completion of the last case scheduled for the day that
might necessitate unplanned residents and staff overtime.
The Residents overtime violates the residency duty hours standard
set by Accreditation Council for Graduate Medical Education
(ACGME). Moreover the Technologists overtime may lower staff
satisfaction and incurs additional avoidable expense to the
department.
Objectives
Introduction
The objective of this study is to apply lean sigma quality
improvement principles in an effort to improve last-case
efficiency in our PET-CT department leading to reduction in
unplanned over time, compliance with residency duty hours,
and increase staff and patient satisfaction.
Conclusion
Systematic study of workflow efficiency and application
practical interventions using quality improvement principles
like lean sigma can significantly enhance efficiency of
imaging departments.
JHU PET-CT Percentage distribution of Last Patient from Sep,
2014 - April, 2015
A lean sigma quality improvement principle that constitutes
five stages namely define, measure, analyze, improve and
control was used. A multi-disciplinary team including Patient
Service Coordinators, Technologists, and physicians formed a
team to assess the problem and propose solutions to improve
last case efficiency in the department. A data collection form
was created to record the completion time for the last case
of the day. At the end of each month these data will be
compared with the computer generated time stamps from the
radiology information system. Then the data will be analyzed
and shared with the staff and management team responsible
to determine and implement the appropriate intervention
required to improve the last case efficiency. This process
continued for six month starting from September, 2014 until
the target goal was achieved in April, 2015.
The percentage of last case completion on or before 5:00 pm showed a 44 % increase from a
baseline of 47% (7) in September, 2014 to 91% (20) in April, 2015. Similarly, cases completed
between 5:01 and 6:00 pm significantly declined from 46% (7) in September, 2014 to 9% (2) in
April, 2015. Whereas the 7% completion rate for the after 6:00 pm was completely eliminated to
zero.
The average last case completion time from September 2014 through April, 2015 was 4:22 pm
with a standard deviation of 9 minutes and 95% confidence interval between (4:04 - 4:40). The
latest completion time was 6:53 and earliest completion time was 12:30. Technologists and
Residents overtime hours decreased from average of 2 hrs. per day from September, 2014 to zero
in April, 2015. On the contrary, patient volume increased by 20 % from September, 2014 to April
2015.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
September October November December January February March April
47%
60%
76%
65%
85%
80%
73%
91%
Before 5:00 5:00-5:30 5:31-6:00 After 6:00
91% of last cases completed
before 5:00 pm by April,
2015.
Patient volume increased by
from September, 2014.
No Staff overtime reported
for the last three months.
I
n
c
r
e
a
s
e
I
n
c
r
e
a
s
e
44 %
Project Charter: System Improvement to Increase Last-Case Efficiency in a busy PET-CT Center Champion:
Rathan Subramanian M.D., Ph.D.
Quality Advisor: Jeff Leal
Problem Statement:
Work flow efficiency is highly impacted by the timeliness of the first-case of the day in a department like PET-CT
that require longer physiological preparation before a scan can be done. Patient scheduling in PET-CT is carefully
designed to avoid camera down time, as soon as a patient scan is completed the next one will follow with in a
minute. Any delay in a patient scan will have a cascade effect on the subsequent scans leading to poor last case
completion rate and unplanned overtime.
Project Goal:
To improve last-case efficiency in PET-CT department from base line of
47 % in September 2014 to 90 % in February 2015.
Project Y / Path-Y:
Percentage of last cases completed before 5:00 pm.
Scope:
First and last case of the day in PET-CT division from September 2014 to
April 2015.
Team Members:
Bineyam Gebrewold: Project leader
Corina Voicu : member (Sr. Technologist)
Esther Mena : member (Physician)
Natarsha Fields : member (PSC)
Benefits:
Minimize unplanned over time.
Compliance with residency duty hours set by ACGME.
Increase staff satisfaction.
Increase patient satisfaction.
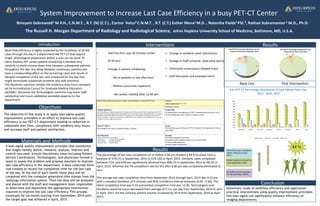
Results
• Start the first case 30 minutes earlier
(6:30 am)
• Change in patient scheduling.
- No in-patients in late afternoon
- Reduce successive inpatients
- No cardiac viability after 12:00 pm.
47%
33%
13%
7%
JHU PET/CT Percentage distribution of Last
Patient Of the Day for September, 2014
91%
9%
0% 0%
JHU PET/CT Percentage distribution of Last
Patient Of the Day for April 2015
• Change in residents work distribution.
• Change in Staff schedule. (Add early techs)
• Eliminated unnecessary delayed scans.
• Staff education and empowerment.
Base Line Post Intervention
Interventions Results
Materials and Methods