Download to read offline





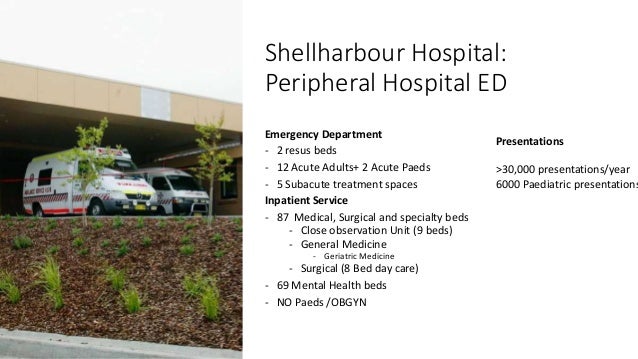





















This was an Orientation talk for new doctors doctors working in Shellharbour ED - expectations and a framework for practice. Shellharbour is a lovely peripheral hospital ED situated in the coastal region of Illawarra NSW. We see >30,000 patients per year, with a broad and interesting range of acuity. Our staff is made up of an interesting mix of local and international doctors who embrace a small hospital team spirit, tackling large hospital problems. Our ED is a mixed adult and paediatric ED that is located 30 mins away from a fully serviced Tertiary hospital. We support ACEM Advanced training with a FACEM led department, supported by ACRRM and Senior CMOs in the medical leadership. The department is host to UOW Clinical Medical students, and subspecialty training term or ED Ultrasound. Our hospital is in the process of an upgrade to include short stay an ICU. The work is challenging but rewarding , and embraces the full mix of what a coast peripheral ED can hope to offer.



























