
Recommended
More Related Content
Similar to Sedative tox.docx
Similar to Sedative tox.docx (20)
Recently uploaded
Recently uploaded (20)
Sedative tox.docx
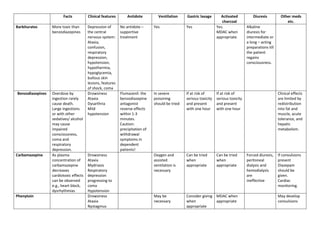
- 1. Facts Clinical features Antidote Ventilation Gastric lavage Activated charcoal Diuresis Other meds etc. Barbiturates More toxic than benzodiazepines Depression of the central nervous system: Ataxia, confusion, respiratory depression, hypotension, hypothermia, hypoglycemia, bullous skin lesions, features of shock, coma No antidote – supportive treatment Yes Yes Yes. MDAC when appropriate. Alkaline diuresis for intermediate or a long – acting preparations till the patient regains consciousness. Benzodiazepines Overdose by ingestion rarely cause death. Large ingestions or with other sedatives/ alcohol may cause impaired consciousness, coma and respiratory depression. Drowsiness Ataxia Dysarthria Mild hypotension Flumazenil: the benzodiazepine antagonist reverse effects within 1-3 minutes. Caution: precipitation of withdrawal symptoms in dependent patients! In severe poisoning should be tried If at risk of serious toxicity and present with one hour If at risk of serious toxicity and present with one hour Clinical effects are limited by redistribution into fat and muscle, acute tolerance, and hepatic metabolism. Carbamazepine As plasma concentration of carbamazepine decreases cardiotoxic effects can be observed e.g., heart block, dysrhythmias Drowsiness Ataxia Mydriasis Respiratory depression progressing to coma Hypotension Oxygen and assisted ventilation is necessary Can be tried when appropriate Can be tried when appropriate Forced diuresis, peritoneal dialysis and hemodialysis are ineffective If convulsions present Diazepam should be given. Cardiac monitoring. Phenytoin Drowsiness Ataxia Nystagmus May be necessary Consider giving when appropriate MDAC when appropriate May develop convulsions
- 2. Hypotension Confusion Hyperactivity TCA Potentially fatal (2.5 to 3.5g of amitriptyline) 60- 70% of fatal cases never reach hospital alive Muscarinic anticholinergic effects: Sinus tachycardia, mydriasis, hallucinations. Histamine receptor antagonism: Sedation, coma. Blockade of adrenergic receptors: Hypotension. Long QT syndrome. Should be given if respiration is impaired. Hypoxic situation - O2 should be given. Hyperventilation is effective for all TCA induced arrhythmias. Consider when appropriate Can be given Diazepam 5 to 10 mg IV slowly for convulsions. drugs for cardiac arrythmias. Cardiac monitoring. Treatment with plasma alkalinization to a pH of 7.50 - 7.55 using sodium bicarbonate. SSRI Recovery complete in 24hrs if the offending medications are discontinued Serotonin syndrome Symptomatic treatment Lithium Most cases arise due to drug interactions or other precipitants; rarely could be due to deliberate overdose. Nausea, vomiting and diarrhea Prolonged QT Hypotension Ataxia Parkinsonism Paralysis, convulsions and coma Hypernatremia Hypokalemia Serum levels (normal 0.4-1.2 mmol/l) if > 2mmol/l serious. Hydrate well & avoid diuretics. Correct fluid & electrolyte imbalance specially Na and K. Consider when appropriate Not effective Hemodialysis in severe status or renal failure. Anticipate and treat renal failure.