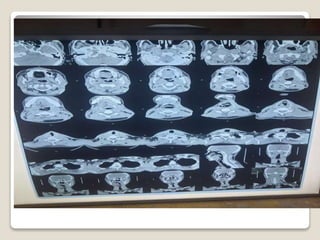
45-year-old male presented with 6 months of progressive right nasal obstruction and blood-stained nasal discharge. He developed right-sided hearing loss and tinnitus 5 months ago. One month ago, he noticed hoarseness of voice, difficulty swallowing, and a painful right neck mass. Examination found restricted movement of the soft palate and right vocal cord with an enlarged right neck lymph node. Differential diagnoses included nasopharyngeal carcinoma and sinus malignancy. CT scan and biopsy were requested to investigate.