LUNGS
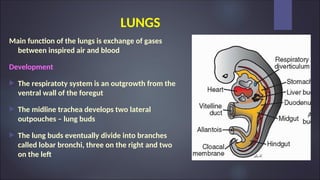
Main function ofthe lungs is exchange of gases
between inspired air and blood
Development
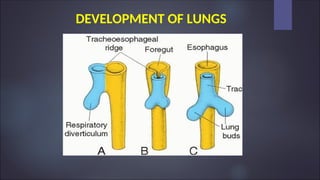
The respiratoty system is an outgrowth from the
ventral wall of the foregut
The midline trachea develops two lateral
outpouches – lung buds
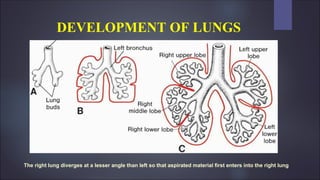
The lung buds eventually divide into branches
called lobar bronchi, three on the right and two
on the left
DEVELOPMENT OF LUNGS
Theright lung diverges at a lesser angle than left so that aspirated material first enters into the right lung
5.
LUNG – NORMALANATOMY
Bronchi have firm cartilagenous walls that provide support and
are lined by columnar ciliated epithelium and with abundant
subepithelial glands that produce mucus
Bronchi branches dichotomously and gives rise to bronchioles
which lack cartilage and submucosal glands in their wall
Bronchioles leads to terminal bronchioles which are less than
2mm in diametre
6.
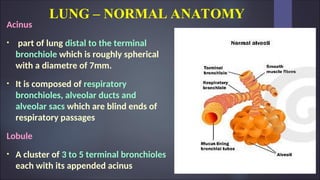
LUNG – NORMALANATOMY
Acinus
• part of lung distal to the terminal
bronchiole which is roughly spherical
with a diametre of 7mm.
• It is composed of respiratory
bronchioles, alveolar ducts and
alveolar sacs which are blind ends of
respiratory passages
Lobule
• A cluster of 3 to 5 terminal bronchioles
each with its appended acinus
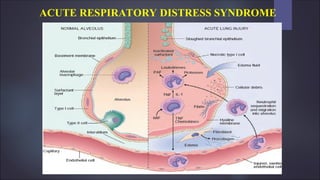
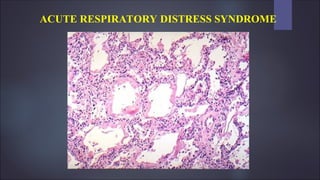
ACUTE RESPIRATORY DISTRESSSYNDROME
ARDS is characterized by abrupt onset of significant
hypoxemia and bilateral pulmonary infiltrates in the
absence of cardiac failure
Associated with inflammation along with increased
pulmonary vascular permeability, edema and epithelial
cell death
ACUTE RESPIRATORY DISTRESSSYNDROME
Pathogenesis
In ARDS the integrity of alveolar capillary membrane formed by two
separate barriers ( microvascular endothelium and alveolar epithelium) is
compromised
ARDS is initiated by injury to pneumocytes and pulmonary endothelium
setting in motion a vicious cycle of increasing inflammation and
pulmonary damage
16.
ACUTE RESPIRATORY DISTRESSSYNDROME
Pathogenesis
After acute insult there is increased synthesis of Interleukin -8 (IL-8)
which is potent neutrophil chemotactic and activating agent
IL-8 and TNF is produced by activated alveolar macrophages
17.
ACUTE RESPIRATORY DISTRESSSYNDROME
Pathogenesis
Endothelial activation
Adhesion and extravasation of neutrophils
Accumulation of intraalveolar fluid and formation of
hyaline membrane
Resolution of injury
18.
ACUTE RESPIRATORY DISTRESSSYNDROME
Pathogenesis
Endothelial activation
It is secondary to pneumocyte injury which activate macrophages
Activated macrophages secrete TNF that act on neighbouring endothelium
Alternatively circulating inflammatory mediators also activate pulmonary
endothelium
Activated endothelial cells express increased levels of adhesion molecules,
procoagulant proteins and chemokines
19.
ACUTE RESPIRATORY DISTRESSSYNDROME
Pathogenesis
Adhesion and extravasation of neutrophils
Neutrophils adhere to the activated endothelium and migrate into
the interstitium and alveoli, where they degranulate and release
inflammatory mediators including proteases, reactive oxygen
species and cytokines
20.
ACUTE RESPIRATORY DISTRESSSYNDROME
Pathogenesis
Accumulation of intra alveolar fluid and formation of hyaline membrane
Endothelial activation and injury make pulmonary capillaries leaky,
allowing interstitial and intraalveolar edema fluid to form
Damage and necrosis of type II alveolar pneumocytes leads to surfactant
abnormalities, further compromising alveolar gas exchange
Ultimately inspissated protein-rich edema fluid and debris from dead
alveolar epithelial cells organize into hyaline membrane, a characteristic
feature of ARDS
21.
ACUTE RESPIRATORY DISTRESSSYNDROME
Pathogenesis
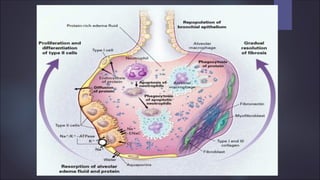
Resolution of injury
When the inflammatory stimulus lessens, macrophages remove
intraalveolar debris and release fibrogenic cytokines such as
transforming growth factor β (TGF-β) and platelet derived growth factor
(PDGF)
these factors stimulate fibroblast growth and collagen deposition,
leading to fibrosis of alveolar walls
Bronchiolar stem cells proliferate to replace pneumocytes
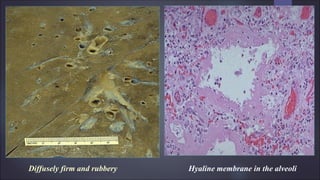
ARDS - MORPHOLOGY
Organizingstage:
Proliferation of type II epithelial cells (to regenerate the alveolar
lining)
Organization of fibrin exudate Intra alveolar fibrosis
Marked thickening of alveolar septa (collagen & proliferation of
interstitial cells)
28.
ACUTE RESPIRATORY DISTRESSSYNDROME
Clinical features
Dyspnea and tachypnea
Cyanosis and hypoxemia
Respiratory failure
Hypoxemia may be refractory to oxygen therapy
LUNG ABSCESS
Theterm pulmonary abscess describes a local suppurative process that
produces necrosis of lung tissue
Commonest organisms isolated from the abscess material are –
- Streptococci
- Staphylococci
- Gram negative organisms
31.
LUNG ABSCESS
Pathogenesis:
Aspirationof infected foreign material: Unconsciousness, Anesthesia,
general debility in which cough reflexes are depressed
Preceding bacterial infection: Bronchopneumonia, Tuberculosis,
Bronchiectasis etc.,
Bronchial obstruction: Bronchial tumor, Foreign body – produces
secondary infection in the obstructed bronchopulmonary segment
Septic embolism: infected emboli from Thrombophlebitis or vegetations
of Infective Bacterial endocarditis
32.
LUNG ABSCESS
Pathogenesis:
Miscellaneous
Directtraumatic injury to lung
Spread of infections from neighbouring organ such as suppuration
in the esophagus, spine, subphrenic space or pleural cavity
Hematogenous seeding of the lung by pyogenic organisms
33.
LUNG ABSCESS
Insome cases no discernible basis for the abscess
formation can be identified – Primary Cryptogenic
abscess
34.
LUNG ABSCESS
Morphology
Size– varies from few mm to large cavities of 5 to 6 cm
Site – may affect any part of the lung and may be single or multiple
Pulmonary abscess due to aspiration are common on the right side and are
single
Abscess which develops in the course of pneumonia or bronchiectasis are
usually multiple, basal and diffusely scattered.
Septic emboli and pyemic abscess – multiple and affect any region of lung
35.
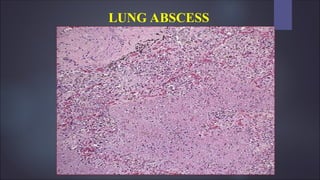
LUNG ABSCESS
Morphology
Abscessis suppurative destruction of the lung parenchyma within central
area of cavitation
Cavity contains suppurative necrotic debris
Continued infection causes multilocular cavities which are poorly
demarcated
Chronic cases fibroblastic proliferation in the fibrous wall abscess occurs
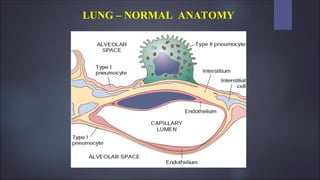
#7 Type I pneumocytes – flat plate like covering 95% of the alveolar surface
Rounded type II pneumocytes – synthesize surfactant which forms a very thin layer over the alveolar cell membranes and are involved in the repair of alveolar damage through their ability to proliferate and give rise to type I cells