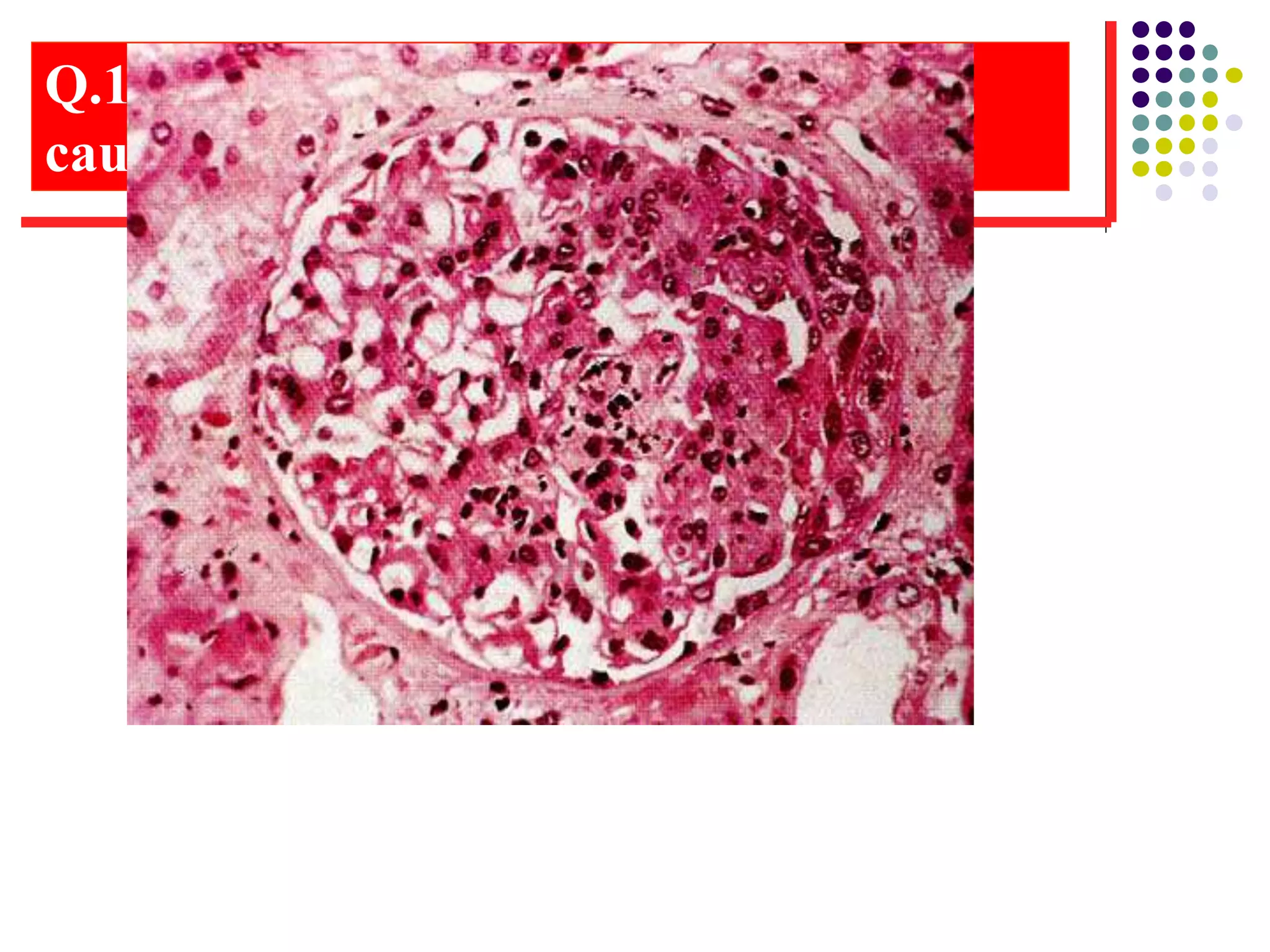
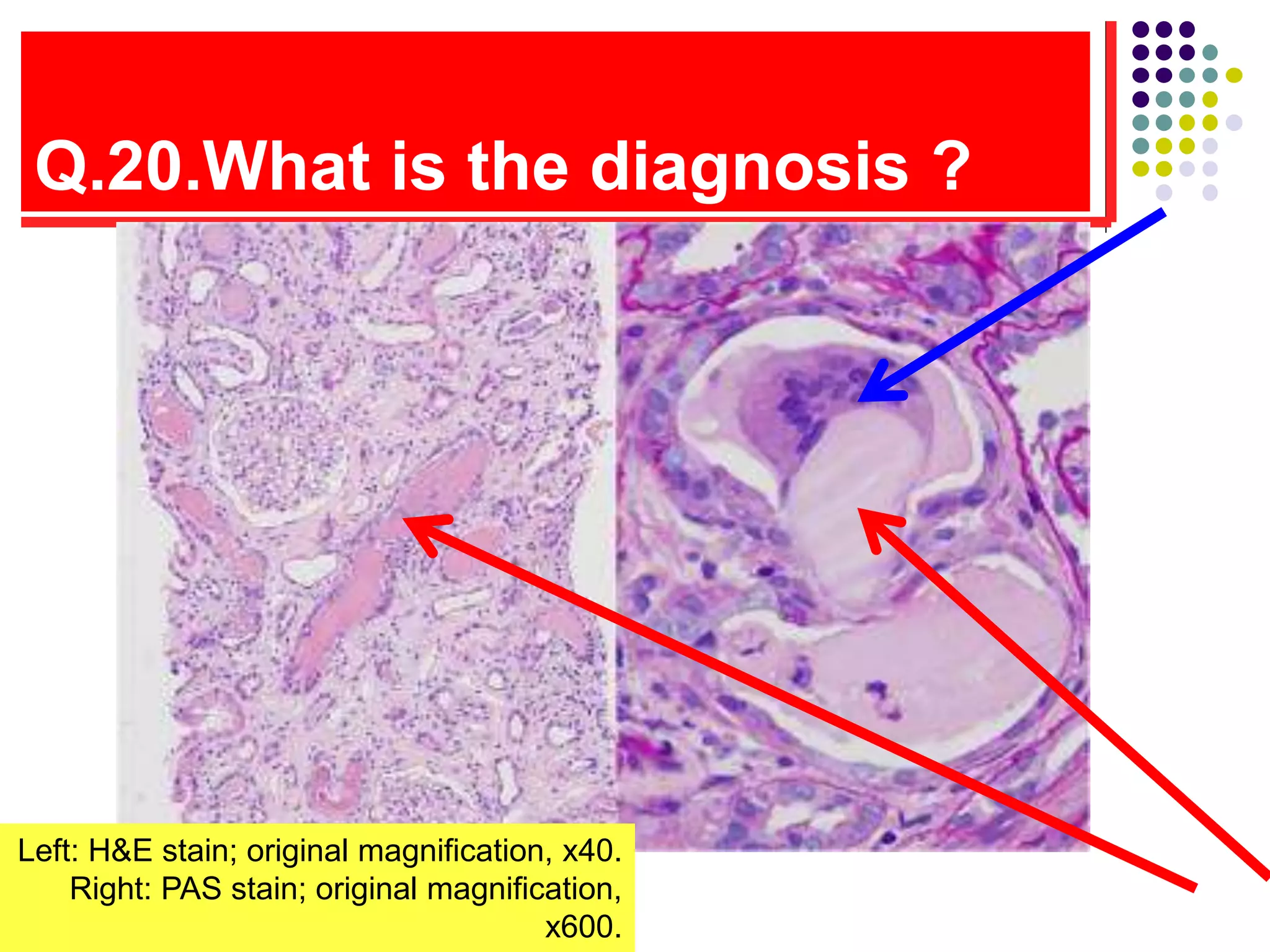
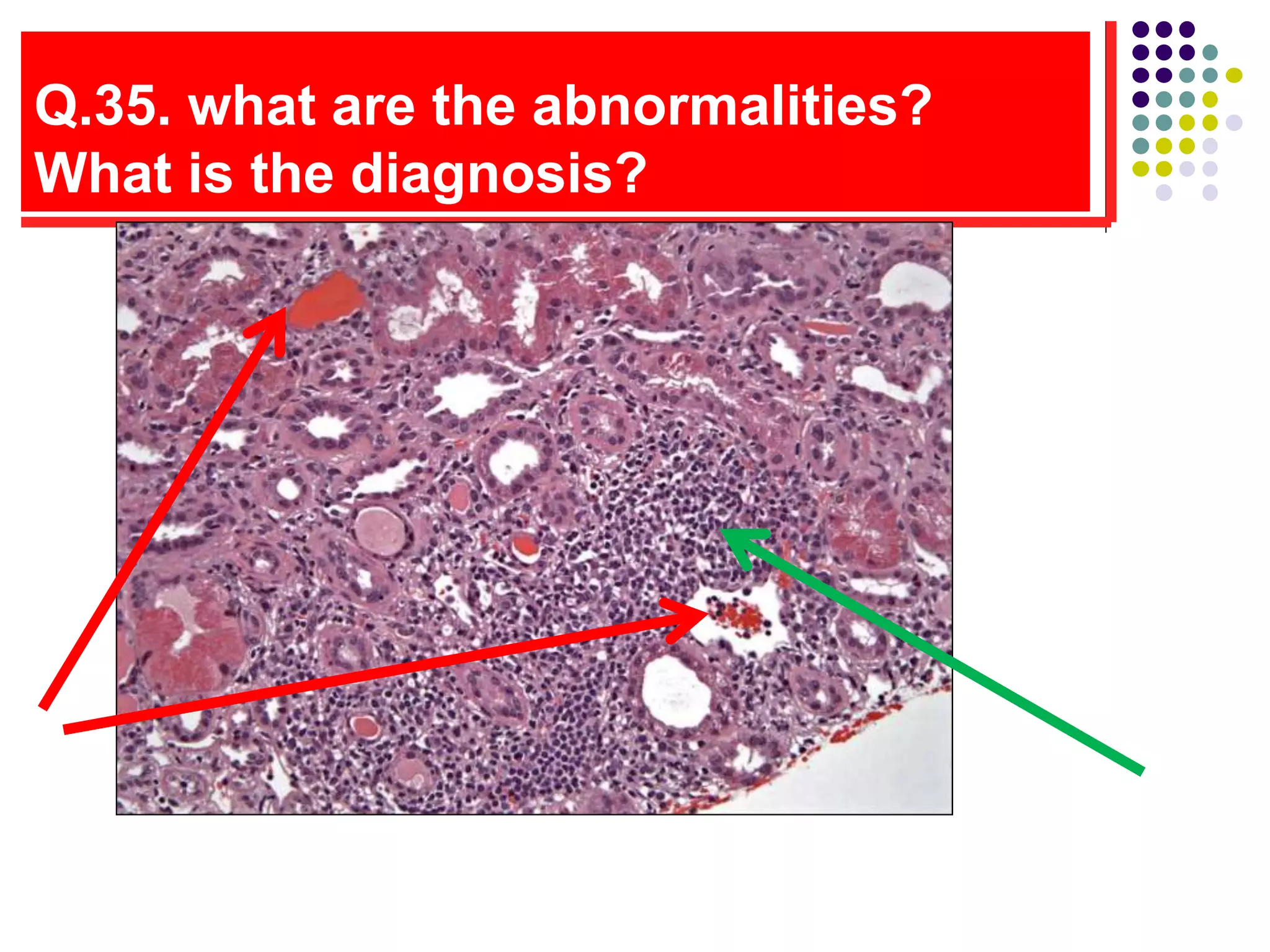
This lesion shows cholesterol emboli in the renal arterioles. Cholesterol emboli, also known as cholesterol crystal embolization syndrome or cholesterol microembolization, is a potential complication of cardiac catheterization where cholesterol crystals break off from atherosclerotic plaques in arteries and become lodged in the arterioles of end organs like the kidneys, causing an inflammatory reaction and fibrosis. The characteristic finding on pathology is biconvex clefts representing dissolved cholesterol crystals surrounded by inflammation.