Drugs play animportant role in the health of both people
and the economy of a country.
Pharmaceutical drugs are available from a large number of
sources.
People and Governments willing to spend money on drugs
for many reasons so, it must be safe, effective and good
quality and used appropriately.
Introduction:
3.
This means, inturn, that development, production,
importation, exportation and subsequent distribution
of drugs must be regulated to ensure that they meet
prescribed standards.
Therefore, effective drug regulation is required to
ensure the safety, efficacy and quality of drugs as well
as accuracy and appropriateness of the drug
information available to the public
4.
Regulatory requirements
►In anideal world, the need for analysis should
be driven by the desire to assure the quality of a
drug product.
►However, in the real world the need for
pharmaceutical drug analysis is driven largely by
regulatory requirements.
►A team consisting of R&D, QC, and QA unit
members develops
these quality and compliance systems.
5.
It should beone of the highest priorities of top
management and QA units to develop and
monitor these systems to comply with the
cGMP and GLP expectations.
Compliance documents are needed, in addition
to the regulatory and research documents, to
demonstrate the integrity of the data.
Compliance documents refer to those reports
required by GMP nd/or utilized during the
course of inspection by a health authority.
6.
Product registration(drug evaluationand authorization,
and monitoring of drug efficacy and safety);
Regulation of drug manufacturing, import, and
distribution;
Regulation & Control of drug promotion and information.
Adverse drug reaction (ADR) monitoring.
Licensing of premises, persons and practices.
Key function of regulatory agencies
Goal of regulatory agency
Main goal of drug regulation is to guarantee the
safety, efficacy and quality of drugs available to
public.
7.
Drug Laws
Drug RegulatoryAgencies
Drug Regulatory Boards
Quality Control
Drug Information Centres etc.
The drug regulations
7
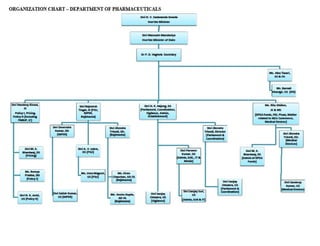
8.
• Department ofPharmaceuticals:
The Department of Pharmaceuticals was created on the 1st of July in
the year 2008 in the Ministry of Chemicals & Fertilizers with the
objective to give greater focus and thrust on the development of
pharmaceutical sector in the country and to regulate various complex
issues related to pricing and availability of medicines at affordable
prices, research & development, protection of intellectual property
rights and international commitments related to pharmaceutical
sector which required integration of work with other Ministries.
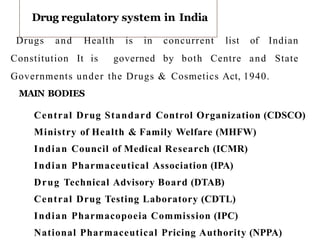
10.
Drug regulatory systemin India
Drugs and Health is in concurrent list of Indian
Constitution It is governed by both Centre and State
Governments under the Drugs & Cosmetics Act, 1940.
MAIN BODIES
Central Drug Standard Control Organization (CDSCO)
Ministry of Health & Family Welfare (MHFW)
Indian Council of Medical Research (ICMR)
Indian Pharmaceutical Association (IPA)
Drug Technical Advisory Board (DTAB)
Central Drug Testing Laboratory (CDTL)
Indian Pharmacopoeia Commission (IPC)
National Pharmaceutical Pricing Authority (NPPA)
1
0
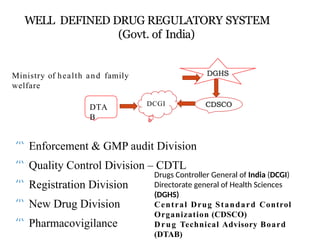
11.
WELL DEFINED DRUGREGULATORY SYSTEM
(Govt. of India)
Ministry of health and family
welfare
Enforcement & GMP audit Division
Quality Control Division – CDTL
Registration Division
New Drug Division
Pharmacovigilance
DCGI
DTA
B
7
Drugs Controller General of India (DCGI)
Directorate general of Health Sciences
(DGHS)
Central Drug Standard Control
Organization (CDSCO)
Drug Technical Advisory Board
(DTAB)
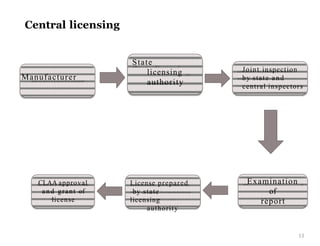
CDSCO
14
Central Drug StandardControl Organization
Head quarters New Delhi
North Zone Ghaziabad
West Zone Mumbai
South Zone Chennai
East Zone Kolkata.
Other zonal offices Ahmedabad and Hyderabad.
Sub-Zonal Office 2
Port offices/Airports 7
Laboratories 6
15.
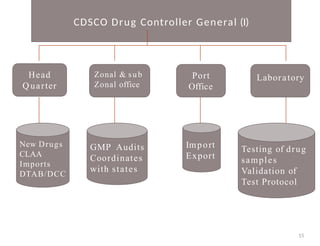
CDSCO Drug ControllerGeneral (I)
15
Head
Q uarter
Zonal & sub
Zonal office
Port
Office
Laboratory
New Drugs
CLAA
Imports
DTAB/DCC
GMP Audits
Coordinates
with states
Import
Export
Testing of drug
samples
Validation of
Test Protocol
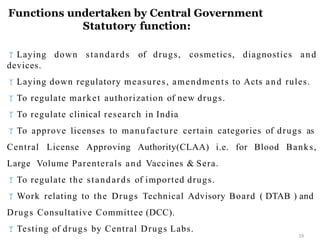
16.
Functions undertaken byCentral Government
Statutory function:
16
Laying down standards of drugs, cosmetics, diagnostics and
devices.
Laying down regulatory measures, amendments to Acts and rules.
To regulate market authorization of new drugs.
To regulate clinical research in India
To approve licenses to manufacture certain categories of drugs as
Central License Approving Authority(CLAA) i.e. for Blood Banks,
Large Volume Parenterals and Vaccines & Sera.
To regulate the standards of imported drugs.
Work relating to the Drugs Technical Advisory Board ( DTAB ) and
Drugs Consultative Committee (DCC).
Testing of drugs by Central Drugs Labs.
17.
National Institute ofHealth and Family Welfare
NIHFW is an Apex Technical Institute, funded by Ministry of
Health and Family Welfare, for promotion of health and family
welfare programmers in the country through education, training,
research, evaluation, consultancy and specialized services.
The NIHFW was established on March 9, 1977 by a merger of
the National Institute of Health Administration and Education
(NIHAE) with the National Institute of Family Planning (NIFP)
NIHF
W
17
18.
18 members
List ofGoverning Body Members of NIHFW
18
NIHFW
1 Chairman
(ex-officio)
1 Vice
Chairman
(ex-officio)
1Member
Secretary
(ex-officio)
9 Member
(ex-officio)
6 Member
19.
Measuring weight ofchildren to assess th e nutritional
status.
Assessment of diseases like level of anemia.
Testing of food material like cooking salt for level iodine.
To release fund on the advice of the Ministry.
It is responsible for all governm ental program s relating
to family planning in India.
ACTIVITIES AND RESPONSIBILITIES
19
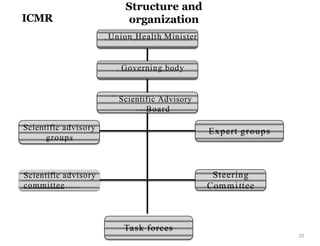
20.
Structure and
organization
20
Union HealthMinister
Governing body
Scientific Advisory
Board
Scientific advisory
groups
Scientific advisory
committee
Expert groups
Steering
Committee
ICMR
Task forces
21.
Extramural research ispromoted by ICMR by establishing
Centers for Advanced Research in different research areas.
Open-ended research is conducted on the basis of
applications for grants-in-aid received from scientists in non-
ICMR Research Institutes, Medical colleges and Universities
located in different parts of the country.
Balancing of research efforts between different competing
fields, especially when resources are severely limited, is a
typical problem encountered in the management of medical
research, particularly in developing countries
ACTIVITIES AND RESPONSIBILITIES
21
22.
IPA
The Indian PharmaceuticalAssociation (IPA) has demanded to
amend the Drugs &Cosmetics Act and Rules 1945 to make only
the pharmacy graduates eligible to become expert staffs in the
pharma manufacturing units.
In the resolutions passed during the just concluded IPA
Convention, the IPA also urged the government to expedite action
to amend the Rules in such way that all regulatory positions in
the country must be an exclusive area for experienced and
qualified pharmacists.
Indian Pharmaceutical Association (IPA) is the premier
professional
association of pharmacists in India.
The association has more than 10,000 members from various
parts of the country and it operates in India through 17 state
branches & more than 33 local branches.
The association represents various facts of pharmaceutical
profession and in managing several academic programmes. 22
23.
DTA
B
23
DTAB
5
Nominated
Members
5 Elected
Members
DRUG TECHNICALADVISORY BOARD
The Central Government constitute a Board (to be called
the Drugs Technical Advisory Board) to advise the Central
Government and the State Governments on technical matters
arising out of the administration of D&C, Act 1940
The Board shall consist of the following members,
– 20 Members
10 exofficio Members
24.
It advices matterrelated to Drugs.
The nominated and elected members of the Board shall hold
office for three years, but shall be eligible for re-nomination and
re-election.
The Board may, subject to the previous approval of the
Central Government, regulating its own procedure.
ACTIVITIES AND RESPONSIBILITIES
24
25.
CENTRAL DRUG TESTINGLABORATORY
The central drug laboratory, Kolkata is national statutory
laboratory of the government of India for quality control of drug
and cosmetic and established under the D&C act ,1940.
Oldest quality control laboratory of the drug control
authorities in India.
Function under the director general of Health Services in
the
Ministry of Health and Family Welfare.
CDTL
25
26.
FUNCTIONS UNDER TAKEN
►Statutory Function :
To Act as an Appellate authority.
To function as Government Analyst for such states who do not
have their own testing facilities.
Analytical quality control of majority of the imported drugs.
Analytical quality control of drug formulations manufactured
within the country on behalf of the Central & State Drug
standard control organization
►Other Functions:
Procurement, establishment, maintenance, Storage and
distribution of I.P & International Reference standards.
Preparation and standardization of I.P. reference standards
against USP, BP primary standards.
To undertake analytical research in standardization and
m2
2 ethodology development of drug.
Development of comprehensivemonographs.
Accord priority to monograph s of drugs included in the
national Essential Drug List and their dosage forms.
Preparation of monograph for products tha t have normally
been in the market for not less than 2 years.
Collaborate with pharmacopoeias like the BP, USP, JP and
International Pharmacopoeia with a view to harmonizing with
global standards.
ACTIVITIES AND RESPONSIBILITIES
28
29.
NPPA National PharmaceuticalPricing Authority
For the purpose of implementing provisions of DPCO, powers of
th e Govern men t have been vested in th e National
Pharm aceutical Pricing Authority (NPPA).
Drugs have been declared as essential and accordingly put unde
the Essential Commodities Act.
Only 74 out of 500 commonly used bulk drugs are kept
under
statutory price control.
However, the prices of other drugs can be regulated, if warranted
in public interest.
The NPPA was established on 29th August 1997 as an
indepen den t body of experts following th e Cabinet
Committee’s d25ecision in September 1994 while reviewing the Drug
Policy.
30.
The Authority, interalia, has been entrusted with the task
of fixation/revision of prices of pharmaceutical products (bulk
drugs and formulations),
enforcement of provisions of the Drugs (Prices Control)
Order
monitoring the prices of controlled and decontrolled drugs in
the country.
NPPA
30
31.
Ceiling and NonCeiling Prices of drugs and medicines in the
controlled category regulated .
Ceiling Price is the single maximum selling price fixed that
is applicable throughout the country in the case of each bulk
drug,which is under price control.
Non-Ceiling Price fixed by NPPA are specific to a particular
pack size of scheduled formulation of a particular company.
Features
31
32.
GMP
Good Manufacturing Pratices
GMP guidelines are not prescriptive instruction s on how to
manufacture products.
They are a series of general principles that m ust be
observed during manufacturing.
When a com pany is setting u p its quality program and
manufacturing process, there may be many ways it can
fulfill GMP requirements.
It is the company's responsibility to determine the most
effective and efficient quality process.
32
33.
To ensurethat their products are safe, pure, and effective.
To minimize or eliminate contamination, mix up and errors.
Issues including recordkeeping, personnel
qualifications, sanitation, cleanliness, equipment verification,
process validation, and complaint Handling.
GMP is also sometimes referred to as "cGMP”.
Failure of firms to comply with GMP regulations can result in very
serious consequences including recall, fines, and even
imprisonment.
REQUIREMENTS
33
34.
WHO GUIDELINES (WorldHealth Organization):
34
Who is an agency of United Nations. It is a specialised agency and
its primary responsibility includes international health matters so
that the goal, health for all, can be achieved.
The WHO GMP and the certification scheme was accepted by WHA
(world health assembly) in solution no WHA 28.65, as the revised
version in 1975.
With appearance of ISO (International Organization For
Standardization) the WHO GMP needed next revision. The revised text
contains 3 parts.
Part I: out lines the general concepts of quality assurance and salient
components of GMP’s.
Part II: outlines on actions to be taken by production & quality
control personnel separately for implementing general principles of
quality assurance.
Part III: supporting and supplementary guidelines.
35.
The revised textof GMP appears as annex.
ANNEX I: Quality Management in the Drug Industry
35
– Philosophy & Essential Elements
Quality Assurance
Good Manufacturing Practice
Quality Control
Sanitation & Hygiene
Validation
Complaints
Product recalls
Contract Production & Analysis
Self inspection and quality
audits
Personnel
Premises
Material
Documentation
36.
ANNEXURE II:
Good Practices– Production & Quality Control
36
Good Practices in Production
Good Practices in Quality Control
ANNEXURE III:
Supporting and Supplementary Guidelines
Sterile pharmaceutical Products
Good Manufacturing Practice for Active
Pharmaceutical Ingredients
37.
WHO GMP
Certification
37
Originally establishedin 1969 and revised in
1975.
Main objectives were :
To inspect drug manufacturing facilities
To assess compliance of GMP
This would facilitate implementation of the scheme.
WHO GMP ensures the following:
Avoidance of Cross- Contamination
Prevention of Mix-ups
Provide Traceability
Accountability of actions
Responsibility
Product Performance Guarantee
38.
DEFINITION
The U.S. Foodand drug administration is an
agency of the United States Department of Health
and Human services and is responsible for the
safety regulation of most type of foods
38
dietary supplements
Drug
Vaccines
Biological medical products
blood products
medical devices
radiation – emitting devices
veterinary products and
Cosmetics
The agency of the U.S. Department of Health and Human
Services.
Established in 1927.
FDA
39.
How does ICHwork?
• The Steering Committee meets at least twice a year .
During these meetings, new topics will be considered
for adoption, reports are received on the progress of
existing topics, and maintenance and implementation
of the guidelines are discussed.
• The topics identified for harmonization by the
Steering Committee are selected from Safety, Quality,
Efficacy, and Multidisciplinary matters. 39
th rough th e ICH Steering
operates administrative Com mittee with support
Coordinators.
fromthe ICH Secretariat and ICH
40.
Your Responsibilities UnderThe Law
1. Before searching any person, explain him that he has a right to
be searched before a gazetted officer or a magistrate. If he so
requires, take him to a gazetted officer or a magistrate before
whom he can be searched. (Section 50.) without giving him a
chance to part with the drug, controlled substance, etc. you
can search him under Section 100 of the Cr. P. C. (Section
50(5) and 50 (6)).
2. Take down any information given by any person in writing
before authorizing a search (Section 41). If the search is under
Section 42, also send a copy of the information taken in
writing or the grounds of belief for search within 72 hours to
your immediate superior officer.
3. Inform the arrested person, as soon as may be, the grounds of
his
3 6
arrest (Section 52 (1)).
41.
4. If aperson is arrested or an article has been
seized under a warrant issued by a magistrate,
forward the person/seized article to that
magistrate (Section 52 (2)).
5. If the person has been arrested or the article has been
seized otherwise than under a warrant , forward it to
the nearest police station or any other officer
empowered under section 53 (Section 52 (3)).
6. If the person has been arrested or the article has
been seized
• otherwise than under a warrant , forward it to the
nearest police station or any other officer empowered
under section 53 (Section 52 (3)).
7. Whenever you arrest any person, make a full report to
your
superior within 48 hours ( Section 57)
42.
1. Officers Officersacting in discharge of their duties in good
faith under the Act are immune from suits, prosecution and
other legal proceedings ( Section 69).
2. Addicts Addicts charged with consumption of drugs (section
27) or with offences involving small quantities will be immune
from prosecution if they volunteer for de addiction. This
immunity may be withdrawn if the addict does not undergo
complete treatment (Section 64 A ).
3. Offenders Central or state governments can tender immunity
to an offender in order to obtain his evidence in the case. This
immunity is granted by the government and not by the court
(Section 64).
4. Minors All offences committed under any law by persons
under the age of 18 will be covered by the Juvenile Persons
(Care and protection) Act. This Act seeks to reform such
juveniles rather than punish them under the respective Acts.
It prevails over any other Act in respect of persons below the
age of 18.
IMMUNITIES IN DRUG CASES
42
43.
1. DRUG REGULATORYAFFAIRS by sachin itkar,
Dr.S.wyavahare
2. www.fda.gov/cder/guidance/index.htm
3. www.fda.gov/cber/cberftp.html.
References
43
Editor's Notes
#11 Drugs Controller General of India (DCGI)
Directorate general of Health Sciences (DGHS)
Central Drug Standard Control Organization (CDSCO)
Drug Technical Advisory Board (DTAB)






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


