Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies
•
0 likes•56 views

Nick H. Kim, MD, Richard N. Channick, MD, and Vallerie V. McLaughlin, MD, prepared useful Practice Aids pertaining to pulmonary hypertension for this CME activity titled "Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies." For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at http://bit.ly/2O9QbOh. CME credit will be available until July 30, 2019.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies
Similar to Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies
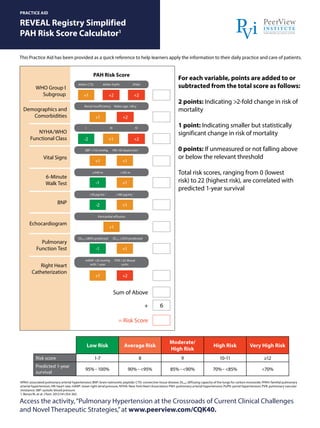
- 1. Access the activity,“Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies,”at www.peerview.com/CQK40. REVEAL Registry Simplified PAH Risk Score Calculator1 PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. APAH: associated pulmonary arterial hypertension; BNP: brain natriuretic peptide; CTD: connective tissue disease; DLCO: diffusing capacity of the lungs for carbon monoxide; FPAH: familial pulmonary arterial hypertension; HR: heart rate; mRAP: mean right atrial pressure; NYHA: New York Heart Association; PAH: pulmonary arterial hypertension; PoPH: portal hypertension; PVR: pulmonary vascular resistance; SBP: systolic blood pressure. 1. Benza RL et al. Chest. 2012;141:354-362. For each variable, points are added to or subtracted from the total score as follows: 2 points: Indicating >2-fold change in risk of mortality 1 point: Indicating smaller but statistically significant change in risk of mortality 0 points: If unmeasured or not falling above or below the relevant threshold Total risk scores, ranging from 0 (lowest risk) to 22 (highest risk), are correlated with predicted 1-year survival Demographics and Comorbidities NYHA/WHO Functional Class Vital Signs 6-Minute Walk Test BNP Echocardiogram Pulmonary Function Test Right Heart Catheterization APAH-CTD I APAH-PoPH III FPAH IV Males age >60 y HR >92 beats/min-1 DLCO ≤32% predicted PVR >32 Wood units <165 m >180 pg/mL-1 Pericardial effusion Renal insufficiency SBP <110 mmHg DLCO ≥80% predicted mRAP >20 mmHg with 1 year ≥440 m <50 pg/mL-1 +1 +1 +1 +1 -1 -2 -1 +1 +1 +1 +1 +1 +2 +1 -2 +2 +2 +2 +2 6 = Risk Score Sum of Above + PAH Risk Score Low Risk Average Risk Moderate/ High Risk High Risk Very High Risk Risk score 1-7 8 9 10-11 ≥12 Predicted 1-year survival 95% - 100% 90% - <95% 85% - <90% 70% - <85% <70% WHO Group I Subgroup
- 2. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension: Diagnostic Algorithm1 Access the activity,“Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies,”at www.peerview.com/CQK40. PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. a CT pulmonary angiography alone may miss diagnosis of chronic thromboembolic pulmonary hypertension. CHD: congenital heart disease; CTD: connective tissue disease; CTEPH: chronic thromboembolic pulmonary hypertension; DLCO: diffusing capacity of the lungs for carbon monoxide; ERS: European Respiratory Society; ESC: European Society of Cardiology; HRCT: high-resolution computed tomography; mPAP: mean pulmonary arterial pressure; PA: pulmonary angiography; PAH: pulmonary arterial hypertension; PAWP: pulmonary artery wedge pressure; PFT: pulmonary function test; PH: pulmonary hypertension; PVOD/PCH: pulmonary veno-occlusive disease/ pulmonary capillary hemangiomatosis; PVR: pulmonary vascular resistance; RHC: right heart catheterization; RV: right ventricular; V/Q: ventilation/perfusion. 1. Galiè N et al; ESC Scientific Document Group. Eur Heart J. 2016;37:67-119. Symptoms, signs, history suggestive of PH Consider left heart disease and lung diseases by symptoms, signs, risk factors, ECG, PFT + DLCO, chest radiograph and HRCT, arterial blood gases Consider other causes and/or follow-up Diagnosis of left heart diseases or lung diseases confirmed? V/Q scana Mismatched perfusion defects? Refer to PH expert center PAH likely Specific diagnostic tests No signs of severe PH/RV dysfunction Treat underlying disease CTEPH possible: CT PA, RHC ± PA RHC mPAP ≥25 mmHg, PAWP ≤15 mmHg, PVR >3 Wood units Signs of severe PH/RV dysfunction Refer to PH expert center Consider other causes Group 5 CTD Drugs – Toxin HIV CHD Idiopathic PVOD/PCH Idiopathic PAH Heritable PAH Heritable PVOD/PCH Porto- pulmonary Schistosomiasis Echocardiographic probability of PH High/intermediate Yes Yes Yes Yes No No No Low
- 3. Access the activity,“Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies,”at www.peerview.com/CQK40. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension: Treatment Algorithm for CTEPH1 PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. a Technically operable patients with non-acceptable risk/benefit ratio can be considered for BPA. b In some centers, medical therapy and BPA are initiated concurrently. BPA: balloon pulmonary angioplasty; CTEPH: chronic thromboembolic pulmonary hypertension; ERS: European Respiratory Society; ESC: European Society of Cardiology; PH: pulmonary hypertension. 1. Galiè N et al; ESC Scientific Document Group. Eur Heart J. 2016;37:67-119. Diagnosis confirmed by CTEPH expert center Lifelong anticoagulation Operability assessment by a multidisciplinary CTEPH team Technically operable Technically non-operable Non-acceptable risk/benefit ratioa Acceptable risk/benefit ratio Pulmonary endarterectomy Persistent symptomatic PH Targeted medical therapy Consider BPA in expert centerb Consider lung transplantation Persistent severe symptomatic PH
- 4. Access the activity,“Pulmonary Hypertension at the Crossroads of Current Clinical Challenges and Novel Therapeutic Strategies,”at www.peerview.com/CQK40. 2015 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension: Treatment Algorithm for PAH1 PRACTICE AID This Practice Aid has been provided as a quick reference to help learners apply the information to their daily practice and care of patients. a Some WHO-FC III patients may be considered high risk. b Initial combination with ambrisentan + tadalafil has proven to be superior to initial monotherapy with ambrisentan or tadalafil in delaying critical failure. c IV epoprostenol should be prioritized as it has reduced the 3-month rate for mortality in high-risk patients with PAH also as monotherapy. d Also consider balloon atrial septostomy. CCB: calcium channel blocker; DPAH: drug-induced pulmonary arterial hypertension; ERS: European Respiratory Society; ESC: European Society of Cardiology; HPAH: heritable pulmonary arterial hypertension; IPAH: idiopathic pulmonary arterial hypertension; PAH: pulmonary arterial hypertension; PCA: prostacyclin analogues; WHO FC: World Health Organization functional class. 1. Galiè N et al; ESC Scientific Document Group. Eur Heart J. 2016;37:67-119. PAH confirmed by expert center Acute vasoreactivity test (IPAH/HPAH/DPAH only) CCB therapy Initial oral combinationb Initial monotherapyb Initial combination including IV PCAc Double or triple sequential combination Consider listing for lung transplantationd Inadequate clinical response Treatment-naïve patient Patient already on treatment General measures Supportive therapy Vasoreactive Non-vasoreactive Inadequate clinical response Consider referral for lung transplantation Low/intermediate risk (WHO FC II-III)a High risk (WHO FC IV)a