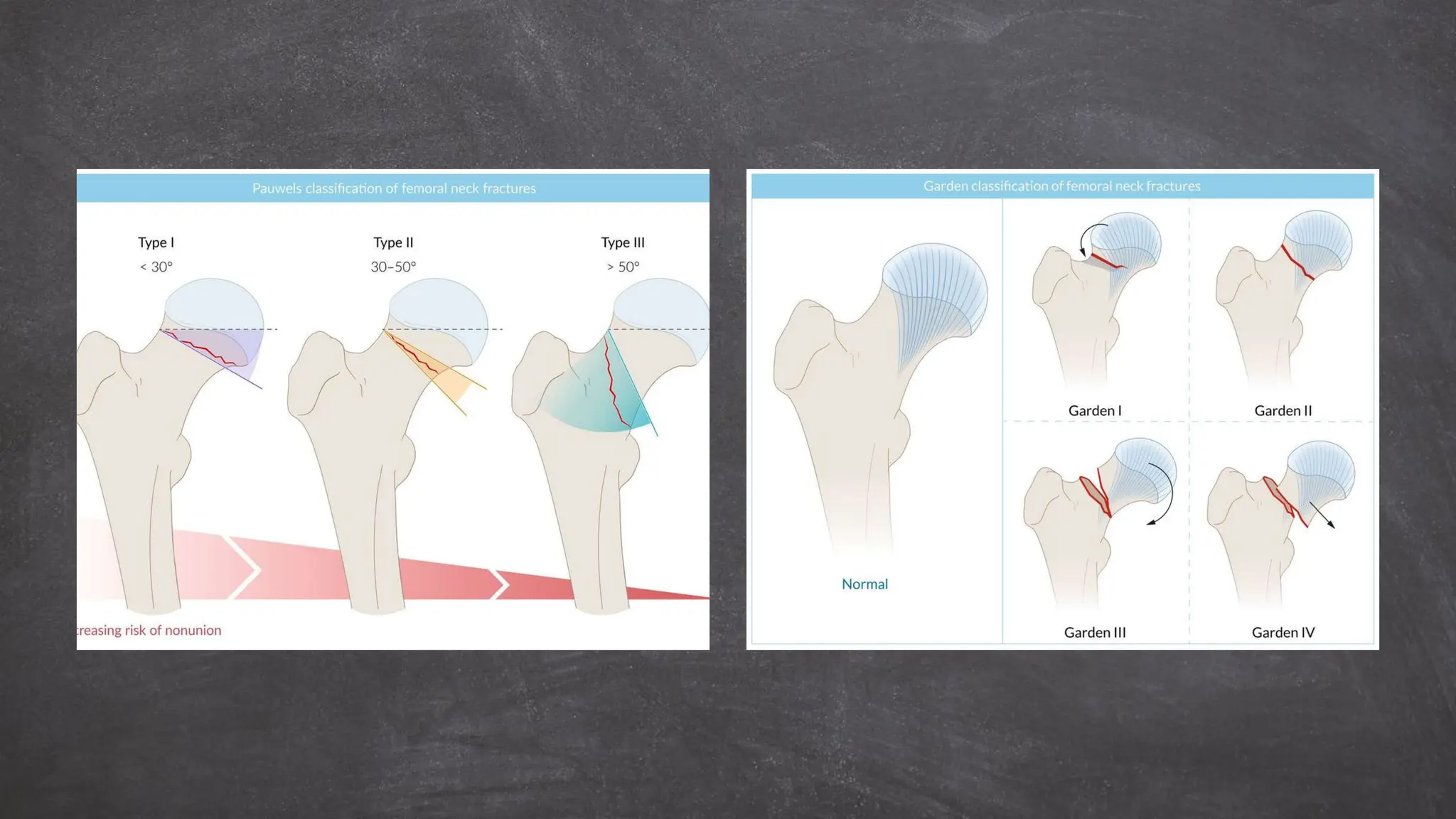
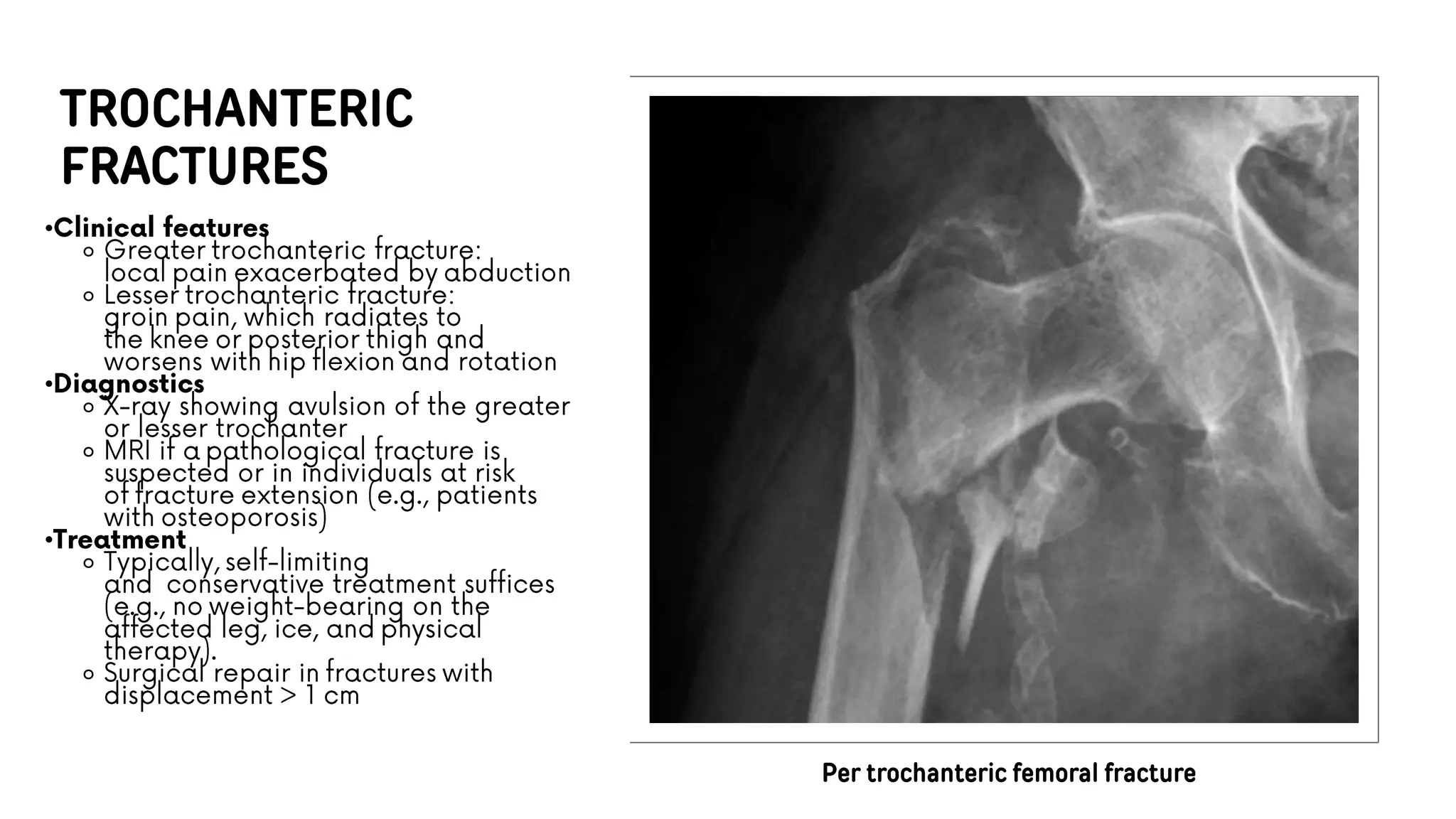
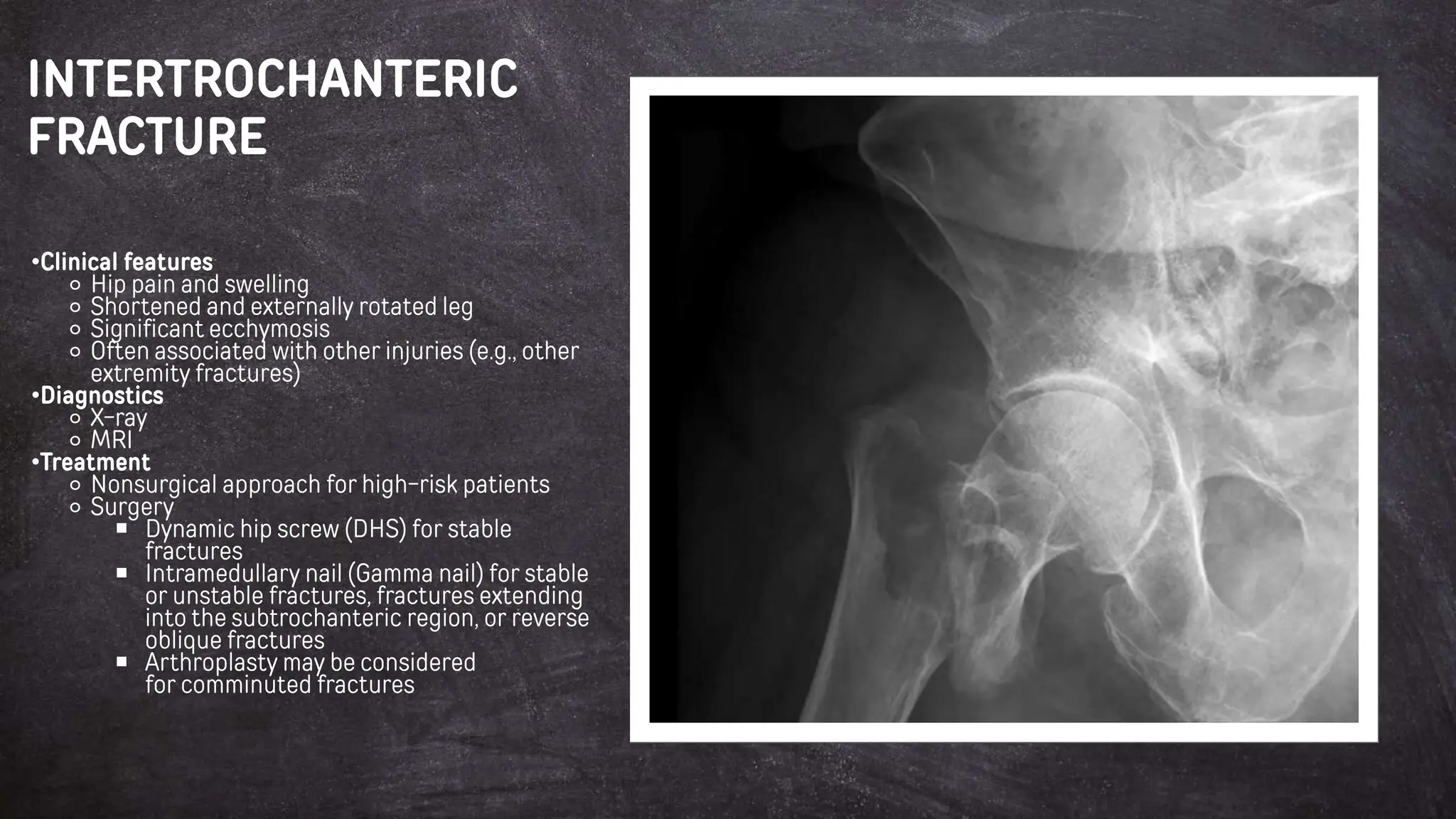
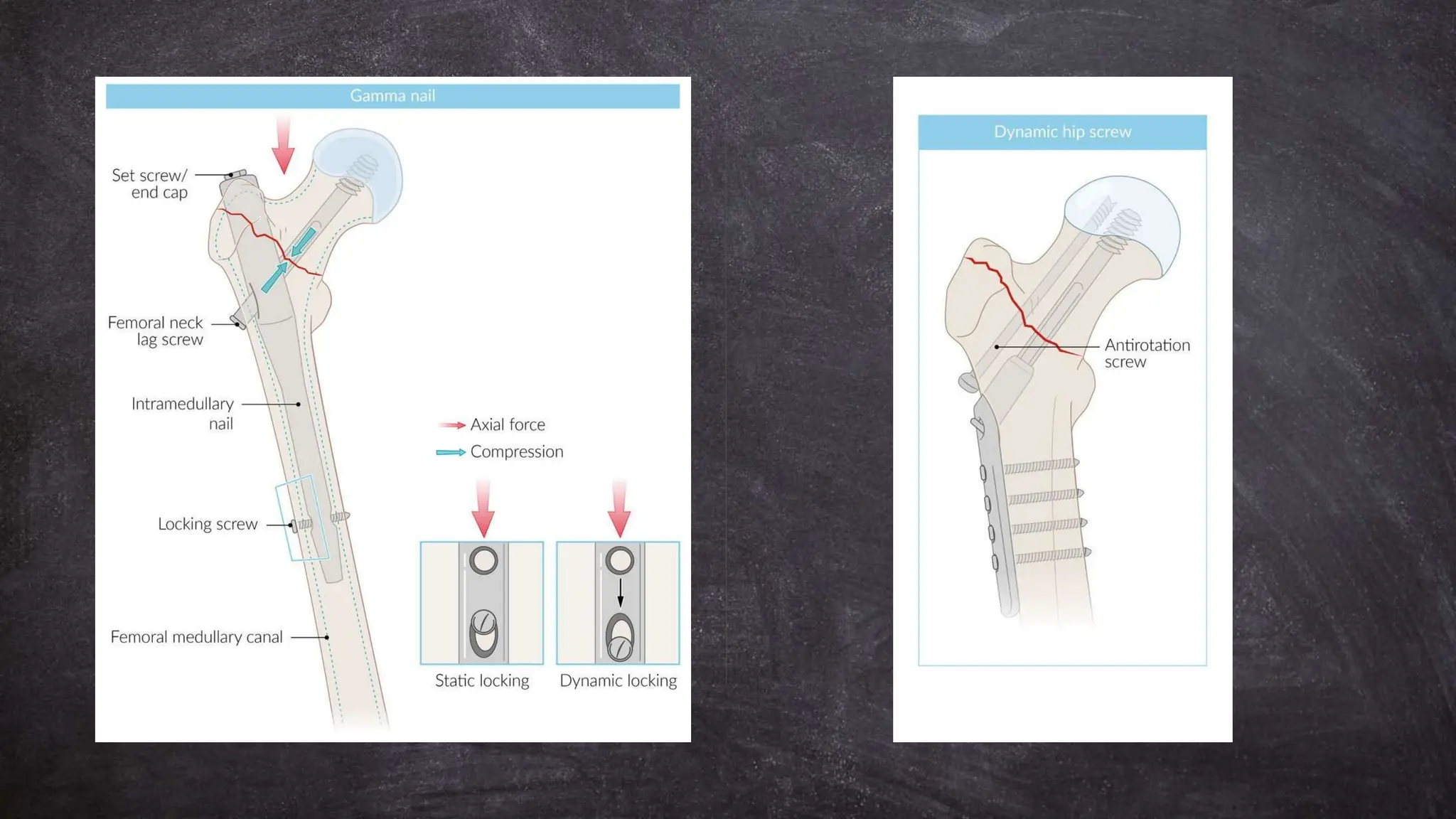
The document outlines the causes, risk factors, clinical features, diagnostics, and treatment options for proximal femoral fractures, which primarily include femoral neck, intertrochanteric, and subtrochanteric fractures. It discusses the mechanics of injury, the classification of fractures, and various surgical and non-surgical options based on patient age and fracture type. It also highlights the importance of considerations such as osteoporosis, muscle weakness, and prior medical conditions in the assessment and management of these fractures.


































![INJURIES AROUND HIP [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/injuriesaroundhipautosaved-240206110505-4ae81da1-thumbnail.jpg?width=640&height=640&fit=bounds)












