Downloaded 26 times




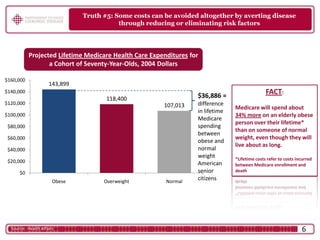


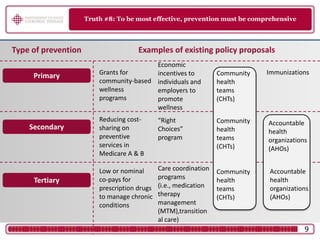

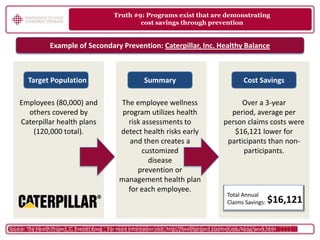





Rising health care spending in the U.S. is largely due to preventable chronic diseases, particularly caused by obesity, with only a small fraction of spending directed towards prevention. There is strong public support for investing in preventive measures in health reform, as many Americans do not receive adequate preventive care, leading to costly health complications. Comprehensive prevention strategies have shown potential for significant cost savings and improved health outcomes.



































































