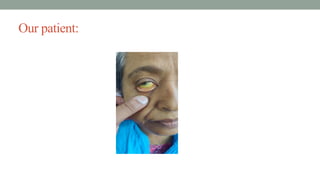
A 56 yearsold female presented with jaundice
Dr. S.M.Arafat
Registrar,department of Hepatology,
Faridpur Medical College Hospital,
Faridpur
2.
Particulars of thepatient
• Name: Mukta Begum
• Age:56 years
• Sex: Female
• Religion: Muslim
• Marital status: Married
• Address: Madhukhali, Faridpur
• Date of admission: 26th
April, 2025
• Date of examination: 26th
April, 2025
3.
Chief complaints:
• Yellowdiscoloration of eyes and urine for 3 weeks
• Generalized itching for same duration
4.
History of presentillness
According to the statement of the patient, she was reasonably well about 3
weeks back. Then she developed yellow discoloration of eyes and urine which
was increasing day by day and not associated with any prodromal features like
anorexia, nausea & vomiting. There was no history of intake of contaminated
water or street food.
She also complained of generalized itching which was more marked at night &
interferes with her sleeping . Her stool is pale colored, voluminous &
occasionally mixed with mucus but not mixed with blood.
She also noticed that a constant dull aching pain at upper abdomen not related
with food intake and relieved after taking meditation.
.
5.
History of presentillness (Continue)
On query she gave history of loss of weight which is not documented but
evidenced by loosening of her cloth.
She has no previous history of fever, Jaundice ,blood vomiting, passage of
black tarry stool, altered behavior, abdominal distension, blood transfusion,
IV drug abuse, any surgery and sexual exposure.
6.
History of pastillness:
• No significant past illness present.
7.
Treatment/drug history
• Patientreceived various medications for her illness from local pharmacy but couldn’t
mention their name. There is no history of taking herbal medications.
8.
Personal history
• Sheis non-smoker and non alcoholic but used to chew betel nuts for a long period.
9.
Socioeconomic history
• Sheused to be a housewife and lives with her son who earns around 30k per month.
She drinks arsenic free deep tubewell water.
10.
Family history
• Herparents and 5 siblings are all healthy. She has 1 son and 1 daughter, both are
healthy. She doesn’t have any family history of liver diseases.
11.
Menstrual/Obstetric history
• Sheis amenorrheic for about 8 years.
• She has two children, both were conducted by NVD and those procedures were
uneventful.
12.
Immunization history
• Sheis not immunized as per EPI schedule, she received three doses of COVID-19
vaccines.
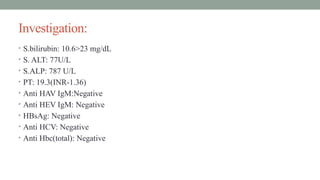
General examination
• Appearance:Illlooking
• Bodybuilt: Below Average
• Nutrition: Average
• Decubitus: On choice
• Anaemia: Mild
• Jaundice: Present(deep)
• Cyanosis: Absent
• Clubbing: Absent, nail is shiny
• Koilonychia: Absent
• Leukonychia: Absent
15.
General examination
• Oedema:Absent
• Dehydration: Absent
• Pigmentation and scratch mark: scratch marks are present all over the body more on
the extensor surface of leg and forearm,no pigmentations
Lymphnode: No lymphadenopathy
• Thyroid gland: Not enlarged
• Bony tenderness: Absent
• Pulse: 80beats/min
• BP: 130/70 mmHg
• Temperature: 99 degree F
• Respiratory rate: 16 breaths/min
16.
Systemic examination
• Gastrointestinalsystem:
• Mouth ans oral cavity: Yellow tinge on ventral surface of tongue.
• Abdomen
• Inspection
• Shape of the abdomen: normal in shape, no distension
• Movement: No visible peristalsis is seen
• Umbilicus is centrally placed and inverted
• Multiple Scratch marks are seen
• No visible veins, pigmentations seen.
17.
Continue
Palpation :
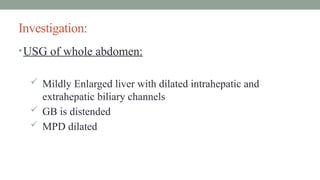
• Liveris enlarged about 4cm from right costal margin along the mid clavicular line,
firm in consistency with smooth surface, sharp margin, non tender. Upper border of
liver dullness is in the right fifth intercostal space in midclavicular line.
• Gall bladder is palpable, smooth surface and non tender
• Spleen is not palpable.
• Hernial orifices are normal on cough impulse
• Per rectal examination not done.
Other system examination:
•Respiratory, Cardiovascular, Nervous ,Musculoskeletal & other system
examination reveals no abnormalities
21.
Salient feature
Mrs MuktaBegum, 56years old non diabetic, non hypertensive lady hailing from
Madhukhalu, Faridpur was admitted in female Hepatology ward, FMCH, with the
complaints of yellow discoloration of eyes and urine which was increasing day by day
and not associated with any prodromal features like anorexia, nausea & vomiting. There
was no history of intake of contaminated water or street food.
She also complained of generalized itching which was more marked at night &
interferes with her sleeping . Her stool is pale colored, voluminous & occasionally
mixed with mucus but not mixed with blood.
She also noticed that a constant dull aching pain at upper abdomen not related with
food intake and relieved after taking meditation.
22.
Salient feature
She alsonoticed that a constant dull aching pain at upper abdomen not
related with food intake and relieved after taking meditation.
On query she gave history of loss of weight which is not documented but
evidenced by loosening of her cloth.
She has no previous history of fever, Jaundice ,blood vomiting, passage of
black tarry stool altered behavior, abdominal distension, blood transfusion,
IV drug abuse, any surgery and sexual exposure.
23.
Salient feature
On generalexamination she is anaemic and icteric, deep jaundice is
present,have shiny nails and scratch marks all over her body.
On examination of abdomen there is hepatomegaly of about 4cm from right
costal margin along the midclavicular line.Upper border of liver dullness is
in 5th
intercostal space in midclavicular line. Gall bladder is palpable. Other
system examination reveals no abnormalities.
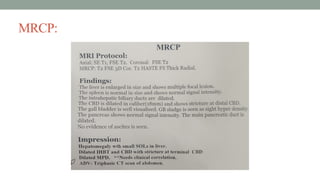
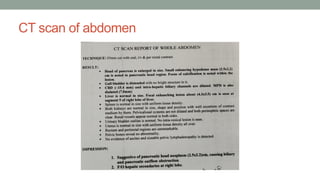
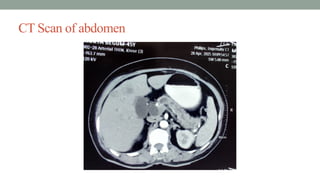
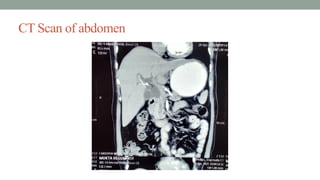
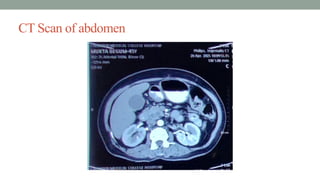
Provisional diagnosis
Obstructive jaundicemost probably due to periampullalry carcinoma
carcinoma of head of the pancreas.
Distal cholangiocarcinoma.
Carcinoma ampulla of vater.
Duodenal growth.
Management
• Diet :Normal.
• Tab. Ursodeoxycholic acid(300) -1+0+1 (A/M)
• Tab. Domperidone(10)-1+1+1 (B/M)
• Inj. Vitamine K -1 amp. I/V daily for 3 days.
• Tab. Tiemonium Methylsulphate – 1+1+1
We consulted with surgery & oncology department for further management.
We also had plan to consult with department of Gastroenterology, but eventually
patient was migrated to Dhaka.