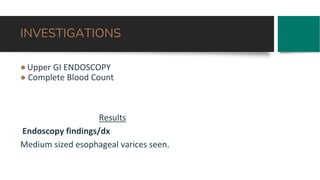
Mr. Kitara Isaac, a 45-year-old male with a history of hypertension, presents with hematemesis and jaundice, having previously been hospitalized for similar complaints. He is diagnosed with liver periportal fibrosis due to schistosomiasis and complicated portal hypertension resulting in esophageal varices. The management plan includes addressing patient concerns, medication like propanolol, and advising for immediate medical attention if symptoms persist.







































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










