
Download to read offline

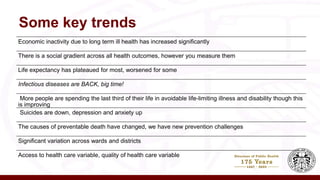
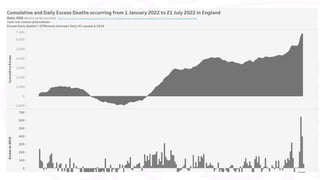

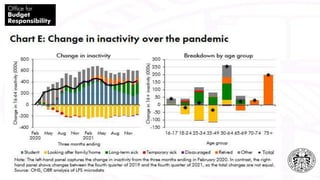
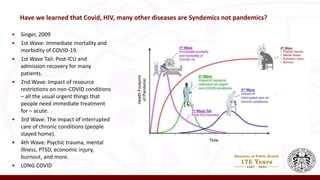

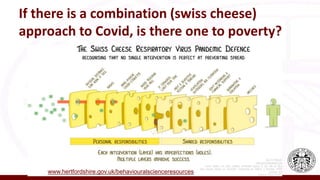
This document discusses the impacts of poverty on health and wellbeing in the context of the COVID-19 pandemic and cost of living crisis. It notes increases in economic inactivity due to long-term illness, worsening life expectancy for some groups, and rising mental health issues like depression and anxiety. It emphasizes that poverty negatively impacts physical, emotional, psychological and social wellbeing. Addressing poverty requires a systems approach that considers socioeconomic factors like income, employment and social support, rather than just focusing on healthcare access. Key strategies discussed include addressing stigma, improving psychological flexibility, and taking a multi-pronged "Swiss cheese" approach similar to COVID-19 responses.



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







