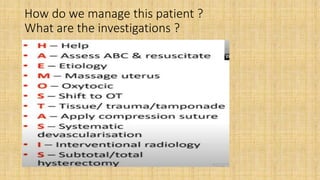
This document discusses two situations involving postpartum hemorrhage:
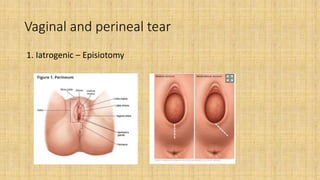
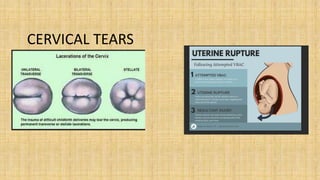
1) Excessive bleeding from the vagina or perineal area, which can be due to tears in the perineal region, vagina, cervix, or uterus. Risk factors include iatrogenic causes like episiotomy.
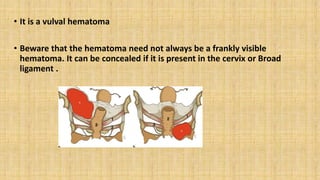
2) Excessive pain in the episiotomy site with no frank bleeding, but low vitals indicating hemorrhage. The cause here is likely a vulval or cervical hematoma that needs to be drained and the source of bleeding ligated and repaired. Management may involve repairing tears, draining hematomas, and identifying and ligating the source of bleeding.