DEFINITION
•Placenta abruption isan abnormal implantation of the
placenta in the lower segment of the uterus near or over
the cervical os instead of attaching to the fundus.
•It is one of the antepartum hemorrhage where the
bleeding occurs due to premature separation of normally
situated placenta.
PATHOGENESIS
• Premature separationis initiated by hemorrhage into the decidua's
basalis.
• The collected blood (decidual haematoma)
• The decidual hematoma may be small and self limited
• If major spiral artery ruptures, a big hematoma is formed.
• As the uterus remains distended by the conceptus, it fails to contract
and therefore fails to compress the torn bleeding points.
6.
RISK FACTORS
The followingare the risk factors associated with Placenta Abruption:
• History of previous placenta previa
• History of previous cesarean birth
• History of prior suction curettage
• Advanced maternal age
• Multifetal gestation, multiparity, or closely spaced pregnancies
• Smoking
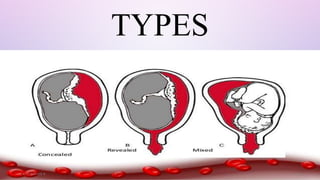
CONCEALED
• The bloodcollect behind the
separated placenta or collected
in between the membranes.
• The collected blood is
prevented from coming out the
cervix by presenting parts on
lower segment.
10.
MIXED
•Some parts ofthe blood collects
inside(concealed) and a part is
expelled out (revealed).
IMMEDIATE DELIVERY
• THEPATIENT IN LABOUR
•LABOUR IS ACCELERATED BY LOW RUPTURE OF THE MEMBRAES,OXYTOCIN DRIP
MAY BE STARTED TO ACCELERATE LABOUR
•VAGINAL DELIVEY IS FAVORED IN CASE WITH
1. PLACENTAL ABRUPTION WITH DEAD FETUS
2. DIC IS PRESENT
• THE PATIENT NOT IN LABOUR
a) INDUCTION OF THE LABOUR
b) CESAREAN SECTION
13.
MANAGEMENT OF
COMPLICATION
•Retro placentalclot is expelled simultaneously with
delivery of baby
•- Oxytocin
•CESAREAN SECTION
• Indications
- Severe abruption with live fetus & very rapid delivery is needed
14.
EXPECTANT
MANAGEMENT
•If bleeding ismild ,no fetal distress , immature fetus
•The goal of the expectant management is prolong the
pregnancy with hope of improving maturity and survival.
•Patient should be monitored in the labour ward for 24-48
hrs to further separation of the placenta may cause fetal
death and maternal complication.
15.
COMPLICATIONS
•MATERNAL COMPLICATIONS:
• ACUTETUBULAR NECROSIS
• COUVELAIRE UTERUS: REFERS TO BLOOD EXTRAVASATING BETWEEN THE
MYOMETRIAL FIBERS.
• POSTPARTUM HEMORRHAGE
• FETO-MATERNAL HAEMORRHAGE.
• MATERNAL MORTALITY
• RECURRENCE: 10% AFTER 1ST ATTACK, 25% AFTER 2ND ATTACK
REFERENCES
• BERGAKKER, S.A. (2010). CASE REPORT: MANAGEMENT OF ELECTIVE CESAREAN
• DELIVERY IN THE PRESENCE OF PLACENTA PREVIAAND PLACENTAACCRETA. AANA JOURNAL,
• 78(5), 380-384.
• CHAMBERLAIN, G. (2006). BRITISH MATERNAL MORTALITY IN THE 19TH AND EARLY 20TH
• CENTURIES. JOURNAL OF THE ROYAL SOCIETY OF MEDICINE, 99(11), 559-563.
• KIM, K. J., & CHA, S. J. (2011). SUPRACERVICAL CERCLAGE WITH INTRACAVITARY
• BALLOON TO CONTROL BLEEDING ASSOCIATED WITH PLACENTA PREVIA. JOURNAL OF
PERINATAL
• MEDICINE, 39, 477-481.