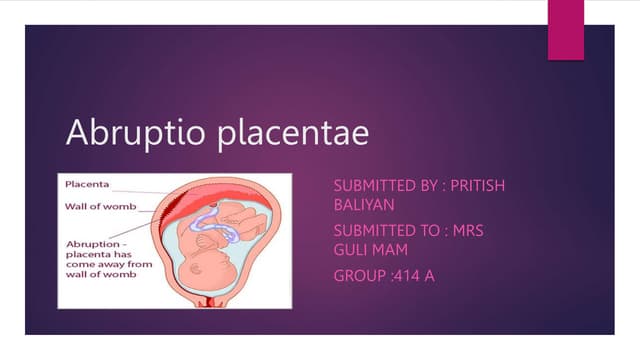
This document discusses the management of preterm labor in cases of placenta previa and abruption placentae. It describes placenta previa as when the placenta is located over or near the internal os, and notes four degrees. For placenta previa, the expectant approach aims to continue the pregnancy for lung maturity using bed rest and monitoring. For abruption placentae, which is premature separation of a normally situated placenta, the active approach is indicated due to risks of further separation and fetal death, with immediate delivery by vaginal or cesarean delivery for severe cases.