10/05/2025
BY ABIE ASCHALE2
CONTENT
Introduction
Risk factors
Pathophysiology
Classification
Diagnosis
Management
Complications
ICU admission criteria and management
3.
10/05/2025
BY ABIE ASCHALE3
OBJECTIVES Define hypertension and PIH
state Risk factors for PIH
Diagnosis of PIH
Classification
Discuss Diagnosis
Discuss Management option for PIH
List the Complications of PIH
Identify ICU admission criteria and
management for PIH
At the end of this session students are expected
to:
4.
10/05/2025
BY ABIE ASCHALE4
INTRODUCTION
What is hypertension ?
Stages of hypertension ?
Types of hypertension?
5.
10/05/2025
BY ABIE ASCHALE5
INTRODUCTION CONTI………
(ACC/AHA) ; 2017
Normal blood pressure Systolic <120 mmHg and diastolic <80 mmHg
Elevated blood pressure – Systolic 120 to 129 mmHg and diastolic <80 mmHg
Hypertension:
•Stage 1 – Systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg
•Stage 2 – Systolic at least 140 mmHg or diastolic at least 90 mmHg
If there is a disparity in category between the systolic and diastolic pressures,
the higher value determines the stage.
6.
10/05/2025
BY ABIE ASCHALE6
Isolated systolic hypertension vs Isolated diastolic hypertension
White-coat hypertension - office/clinic BP (≥140/90 mmHg), but
normal at home or work.
Masked hypertension - BP is normal at a clinic or office visit but
elevated at other times,
more difficult to diagnose- WHY
most typically diagnosed by 24-hour ABPM or automated home
BP monitoring
INTRODUCTION CONTI………
7.
10/05/2025
BY ABIE ASCHALE7
PIH
Pregnancy induced hypertension is defined as a rise in BP> 140/90 mmHg
after the 20th week of gestation measured twice at least six hours apart or a
single measurement of diastolic BP>110mmHg.
Exception
Gestational Trophoblastic diseases (GTD) and multiple pregnancy. Why ?
8.
10/05/2025
BY ABIE ASCHALE8
unique to human pregnancy(PE)
Complicates 7-10% of pregnancies
70% Preeclampsia-eclampsia
30% Chronic hypertension
Eclampsia 0.05% incidence
20% of Maternal Deaths
Cause of 10% of Preterm birth
Etiology unknown
INTRODUCTION CONTI………
9.
10/05/2025
BY ABIE ASCHALE9
RISK FACTORS
A past history of preeclampsia
Multifetal pregnancy - 20 percent
Nulliparity –
family history
Advanced maternal age < 18 or < 35 yrs.
Pre- existing medical conditions:
Pregestational diabetes
underlying kidney or vascular
disease
Obesity
abnormal lipid metabolism
Chronic hypertension
10.
10/05/2025
BY ABIE ASCHALE10
PATHOPHYSIOLOGY
The pathophysiology of preeclampsia likely involves both maternal and
fetal/placental factors
Abnormal development of the placenta
Immunologic factors
Genetic factors
Environmental and maternal susceptibility factors
Preexisting maternal vascular/metabolic/kidney/autoimmune disease
11.
11
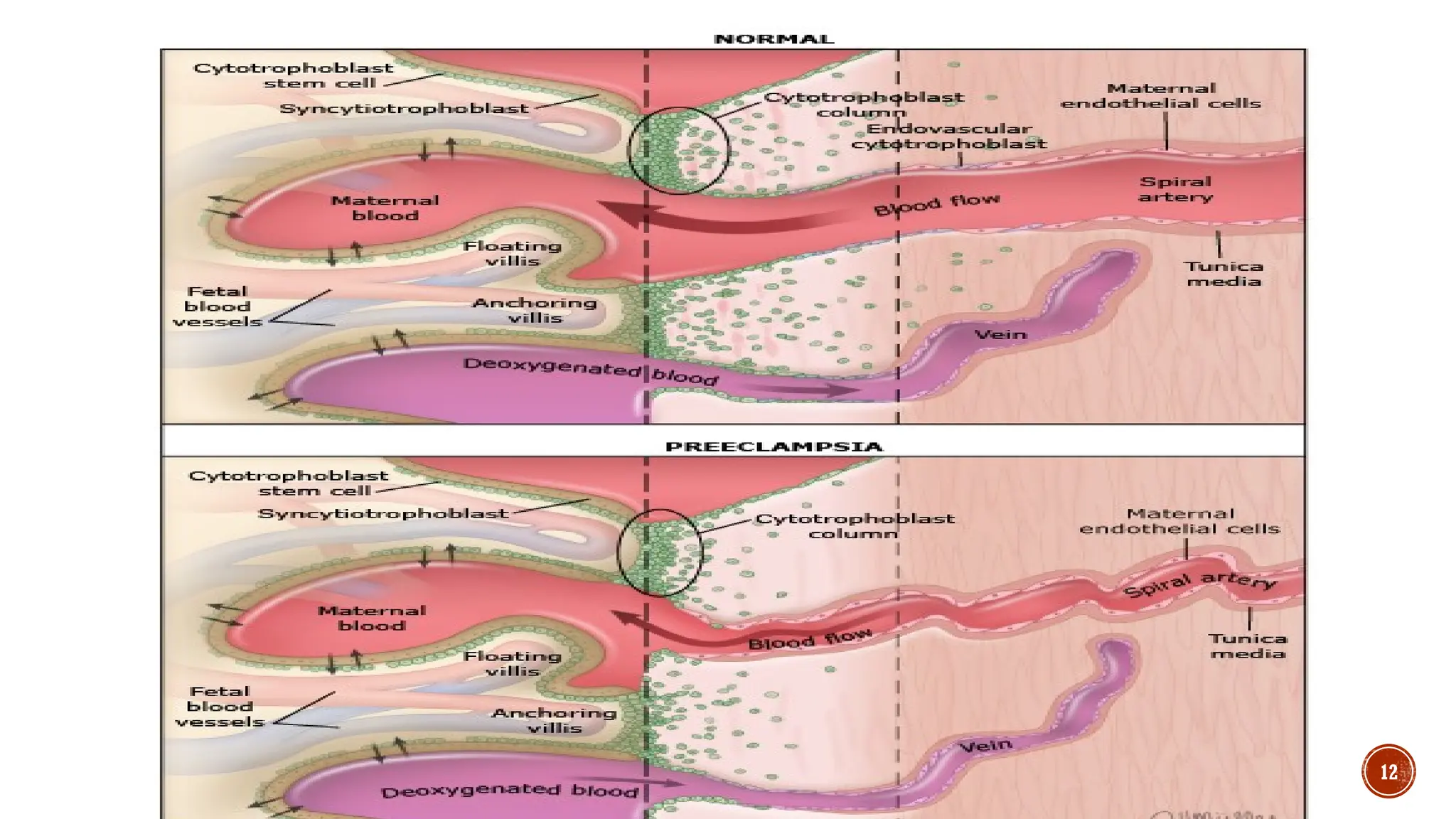
Anormal invasion ofthe spiral arterioles by the cytotrophoblast cells reduced
uteroplacental perfusion placental ischemia (lack of oxygen and nutrients) release
of placental factors endothelial dysfunction in the maternal circulation
Endothelial dysfunction inner lining of the blood vessels becomes impaired and unable to
produce enough vasodilators (substances that relax the blood vessels) such as nitric
oxide and prostacyclin. This results in increased vascular resistanceandhypertension
Endothelial dysfunction to increased production of vasoconstrictors (substances that
narrow the blood vessels) such as endothelin and thromboxane increase the sensitivity of
the blood vessels to angiotensin II, a hormone that regulates blood pressure and fluid
balance
10/05/2025
BY ABIE ASCHALE13
• The increased vascular resistance and hypertension affect the renal
function and cause proteinuria (protein in the urine), edema (swelling),
and reduced glomerular filtration rate (GFR).
• The increased blood pressure and endothelial dysfunction also affect
the brain, the liver, and the coagulation system.
• The placental ischemia and the maternal hypertension also affect the fetal
growth and development. The reduced blood flow and oxygen delivery to the
placenta can cause intrauterine growth restriction (IUGR), fetal distress,
and premature birth image
10/05/2025
BY ABIE ASCHALE16
1. GESTATIONAL HYPERTENSION
BP > 140/90 or more after the 20th week of gestation
without significant proteinuria.
Gestational hypertension may represent pre-eclampsia prior to
proteinuria or chronic hypertension previously unrecognized
17.
10/05/2025
BY ABIE ASCHALE17
2. PRE-ECLAMPSIA
Pre-eclampsia BP > 140/90mmHg
Presence of significant proteinuria of > 300 mg/24 hours urine
specimen OR > 1+ protein (equivalent to approximately 100mg/dl)
on dipstick in at least two randomly collected urine specimen at least 6
hours apart
Based on degree of hypertension or proteinuria and involvement of
other organ systems
18.
10/05/2025
BY ABIE ASCHALE18
1. Mild pre-eclampsia
The mild form of pre-eclampsia is diagnosed when the Systolic and
diastolic blood pressure is between 140-160 and 90-110mmHg respectively
without signs of severity.
19.
10/05/2025
BY ABIE ASCHALE19
2. Severe pre-eclampsia
Severe blood pressure elevation: BP > 110 ∕160mmHg measured twice at
least six hours apart OR A single measurement of diastolic BP
>120mmHg
Proteinuria > 5gm/24 hours or >3+ in randomly collected urine
Pulmonary edema
• Kidney function impairment- Serum creatinine >1.1 mg/Dl
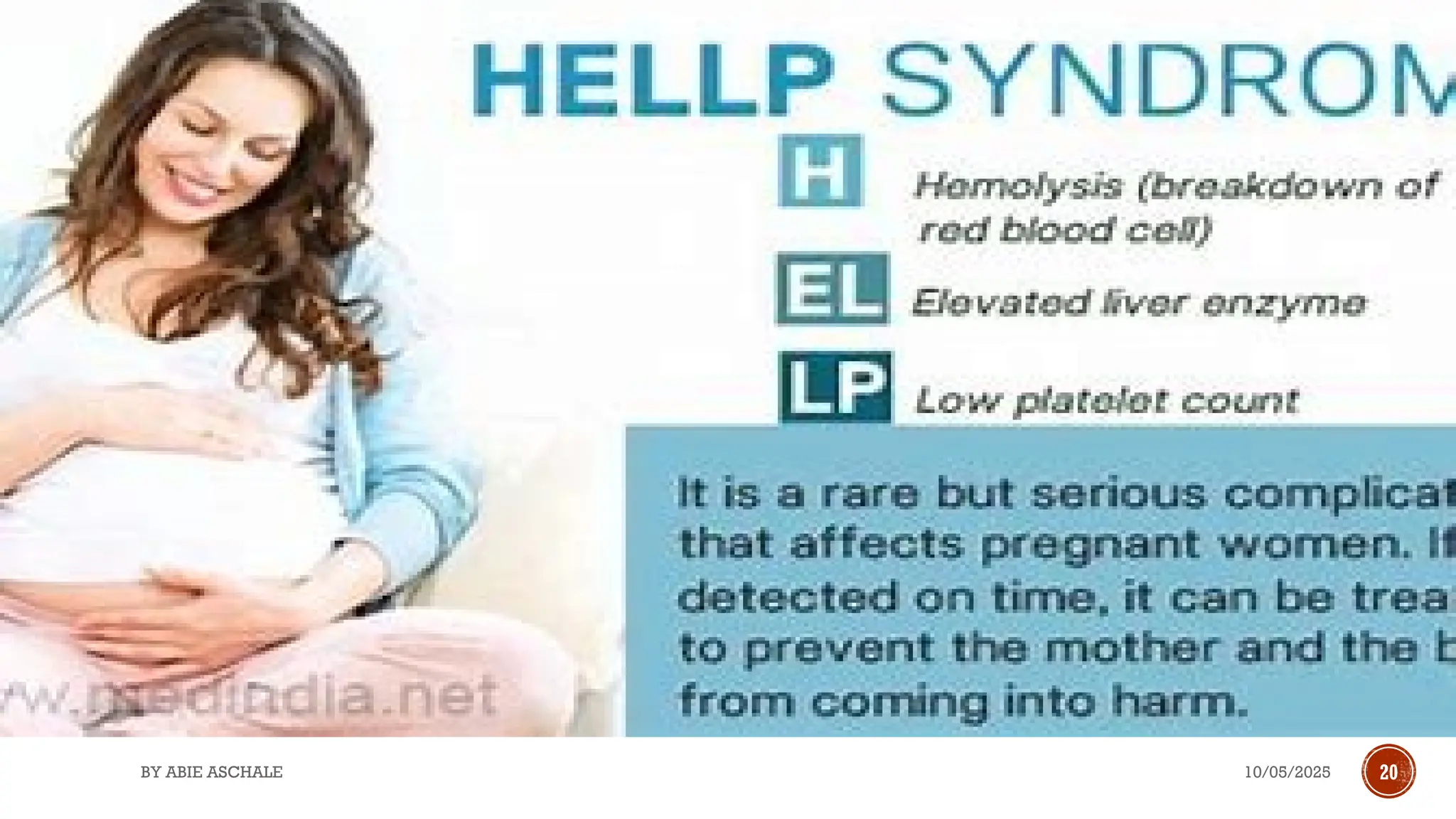
• HELLP syndrome
10/05/2025
BY ABIE ASCHALE21
Elevated Liver Enzymes (HELLP syndrome)
- Disseminated intravascular coagulation (DIC)
- Headache, visual disturbance and right upper abdominal pain
- Oliguria (<400ml in 24hours or 30ml/hour)
- Intrauterine growth restriction (IUGR)
- Cardiac decompensation, Pulmonary edema, cyanosis
22.
10/05/2025
BY ABIE ASCHALE22
3. ECLAMPSIA
Eclampsia is the development of new-onset seizures (generalized tonic clonic type),
superimposed upon
Preeclampsia, in a woman between 20 weeks of gestation and 4 weeks postpartum.
Eclampsia is the convulsive manifestation of preeclampsia
absence of other causative conditions (eg, epilepsy, cerebral arterial ischemia and
infarction, intracranial hemorrhage, drug use
Any convulsion occurring during pregnancy is eclampsia unless proven otherwise
.
10/05/2025
BY ABIE ASCHALE24
MANAGEMENT
objectives
1. Control hypertension
2. Prevent convulsion
3. Prevent complication
4. Deliver viable fetus
25.
10/05/2025
BY ABIE ASCHALE25
GENERAL PRENCIPLES
Stabilization of air way, breathing and circulation is the initial step.
Always anticipate difficult airway in pregnant patients.
Two large-bore intravenous cannula (14G or 16G) should be placed to
administer fluids.
The Foley catheter should be placed to monitor urine output.
Nurse in the left lateral position (30° wedge to the right hip) to prevent supine
hypotension syndrome
26.
10/05/2025
BY ABIE ASCHALE26
Non pharmacologic
- Bed rest at home in the lateral decubitus position.
- Frequent evaluation of fetal well being
- Maternal well being i.e. BP, laboratory
- Advise patient to immediately report whenever they develop symptoms of severity such as
headache, epigastric pain, blurring of vision etc
- Plan termination of pregnancy at term.
- If the disease progresses to severe range, manage as severe case.
Management of mild pre-
eclampsia
Most patients are asymptomatic and can be managed conservatively. Such patients are
not candidates for urgent delivery.
27.
10/05/2025 27
Pharmacologic
BY ABIEASCHALE
BP control
Arterial pressure not greater than 160/110 mmHg in preeclampsia can increase
the risk of complication, and it should be controlled.
Goal of BP control is 15–25% reduction in the mean arterial pressure, and
Reduction of pressure to normal levels (<140/90 mmHg) should be avoided as
it may compromise placental perfusion.
Methyldopa, 250-500mg P.O., 8 to 12 hourly
Nifedipine, 10-40mg P.O., BID OR slow release 30-60mg daily
N.B. Advise patient
10/05/2025
BY ABIE ASCHALE29
1. Labetalol
Dosage
20 mg IV gradually over 2 minutes.
• If BP remains above target level at 10 minutes, give 40 mg IV over 2 minutes.
• If BP remains above target level at 20 minutes, give 80 mg IV over 2 minutes.
Cumulative maximum dose is 300 mg. If target BP is not achieved, switch
to another class of agent. Hold dose if heart rate <60 beats per minute.
A continuous IV infusion of 1 to 2 mg/minute can be used instead of
intermittent therapy or started after 20 mg IV dose.
30.
10/05/2025
BY ABIE ASCHALE30
2. HYDRALAZINE
Repeat BP measurement at 20-minute intervals:
•If BP remains above target level at 20 minutes, give 5 or 10 mg IV over 2
minutes, depending on the initial response.
Cumulative maximum dose is 20 to 30 mg per treatment event.
Initial dose - 5 mg IV gradually over 1 to 2 minutes.*
Less predictable than with IV labetalol.
31.
10/05/2025
BY ABIE ASCHALE31
3. NIFEDIPINE*
Immediate release- 10 mg orally.
• Repeat BP measurement at 20-minute intervals:
• If BP remains above target at 20 minutes, give 10 or 20 mg orally,
depending on the initial response.
• If BP remains above target at 40 minutes, give 10 or 20 mg orally,
depending on the previous response.
33
FIRST LINE -Magnesium sulphate
A loading dose
4gm as 20% solution IV over 10-15 minutes followed by
10gm as 50% IM injection divided on two sides of the buttock,
Maintenance dose
5gm every 4 hours as 50% concentration over 2minutes,
2gm IV as 50% solution over 2minutes if convulsion recurs.
Reduce the maintenance dose by half if there are signs of renal derangement
during labor and for the first 24 hours postpartum
34.
10/05/2025
BY ABIE ASCHALE34
Monitor toxicity
Loss of deep tendon reflexes
Respiratory depression
Loss of patellar reflex
If seizures recur while the patient is receiving magnesium, a repeat (2g)
bolus of magnesium may be given.
Infusion dose should be reduced in case of renal dysfunction.
Serum magnesium level should be monitored
Discontinue magnesium sulfate 24 h after delivery or after last seizer
10/05/2025
BY ABIE ASCHALE40
ICU ADMISSION CRITERIA FOR SEVER CONDITIONS
The criteria for ICU admission for preeclampsia and depending on
the severity of the condition,
the availability of resources, and
the clinical judgment of the obstetrician and the intensivist.
41.
10/05/2025
BY ABIE ASCHALE41
some common indicators may warrant ICU admission are
BP > 160/110 mmHg or higher, despite adequate antihypertensive therapy.
Severe proteinuria (> 4+ on dipstick or 5 g in 24 hours).
Oliguria (UO < 20-30 ml/hr) or AKI (cr. >1.3 mg/dl).
Signs of HELLP syndrome
Epigastric pain, headache, visual disturbances, or altered mental status (signs of
cerebral edema or ischemia).
Seizures or coma (eclampsia).
Pulmonary edema, signs of fluid overload or cardiopulmonary dysfunction.
Fetal distress or IUGR (signs of placental insufficiency or abruption).
42.
10/05/2025
BY ABIE ASCHALE42
GOAL OF ICU CARE AND ROLE OF NURSE
• Blood pressure control with intravenous antihypertensive a
• Magnesium sulfate infusion for seizure prophylaxis and treatment
• Fluid management with careful assessment of the fluid balance, urine
output, and hemodynamics.
• Fetal monitoring with continuous cardiotocography, ultrasound, and
biophysical profile
• Steroid administration for fetal lung maturation if the gestational age is
less than 34 weeks and delivery is anticipated within 7 days.
43.
10/05/2025 43
SUMMERY
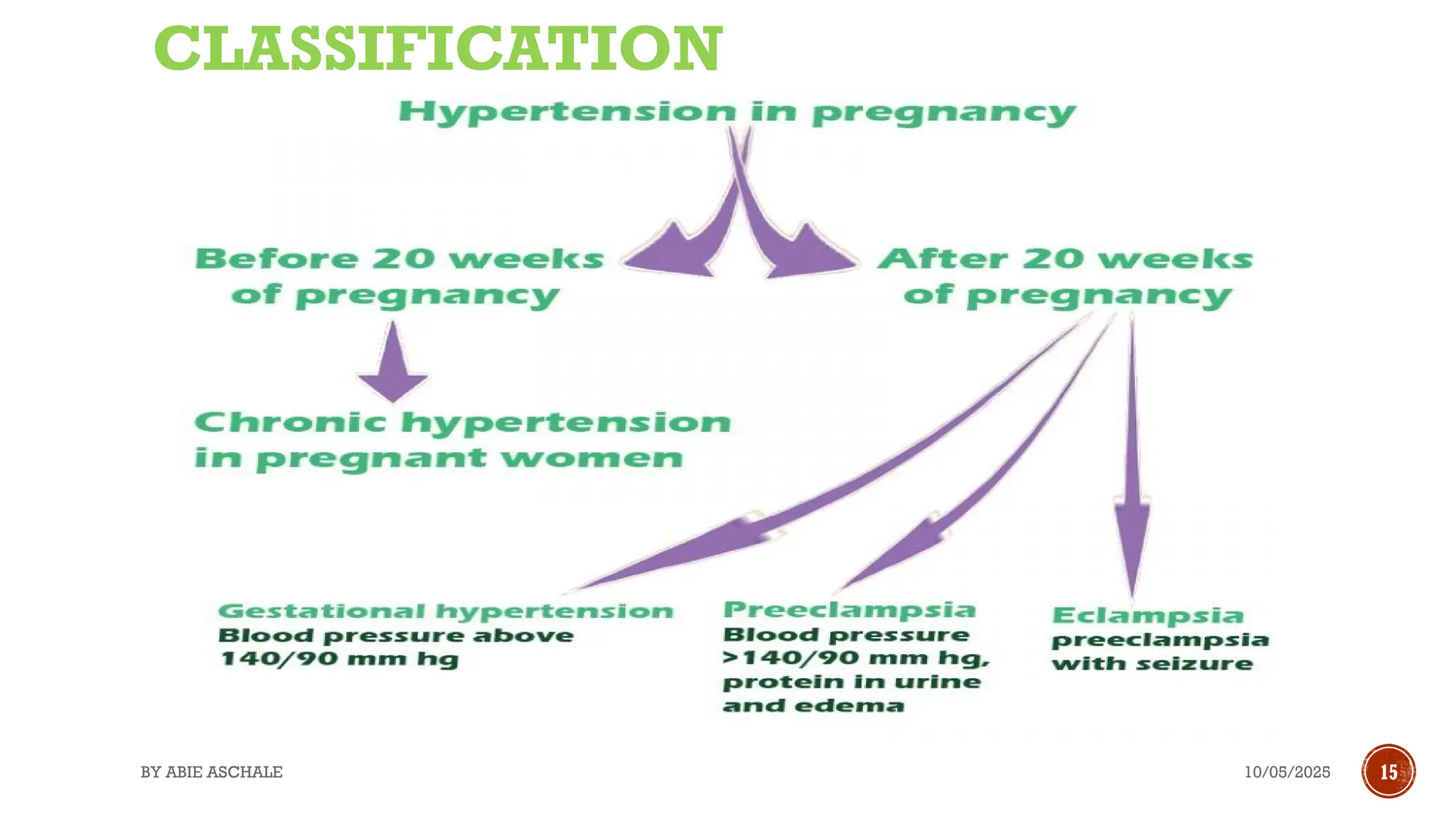
PIH) acondition where a pregnant woman develops high blood pressure after 20 weeks of
pregnancy.
It can affect the mother’s organs and the baby’s growth and development.
PIH can also lead to serious complications such as pre-eclampsia, eclampsia, and HELLP
syndrome.
PIH is diagnosed by measuring blood pressure and checking for protein in the urine.
Treatment options depend on the severity of the condition and the stage of pregnancy. Some
common treatments include bed rest, medication, and early delivery.
PIH usually goes away after childbirth
44.
10/05/2025
BY ABIE ASCHALE44
REFERENCES
Overview of pregnancy induced hypertension– UpToDate,2024
Protocol R. 3: Classification of hypertension in pregnancy. 2012;
Melkie DA, Internist, Teferra DE, Pediatrician, Assefa DM, Oncologist, et al. Food , Medicine and Healthcare Administration
and Control Authority of Ethiopia Standard Treatment Guidelines For General Hospital Diseases Investigations Good
Prescribing & Dispensing Practices for Better Health Outcomes. Fmhaca Addis Ababa. 2014;(3):360.
Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S, et al. Hypertensive disorders of pregnancy: ISSHP
classification, diagnosis, and management recommendations for international practice. Hypertension. 2018;72(1):24–43.
Braunthal S, Brateanu A. Hypertension in pregnancy: Pathophysiology and treatment. SAGE Open Med. 2019;7.
Gouveia, I., Costa, C., Cunha, P. et al. Pre-eclampsia in the intensive care unit: indicators of severity and hospital
outcome. Crit Care 9 (Suppl 1), P216 (2005). https://doi.org/10.1186/cc3279
#31 * We caution against use of immediate-release oral nifedipine, although some obstetric guidelines have endorsed its use as a first-line option for emergency treatment of acute, severe hypertension in pregnancy or postpartum (other options were labetalol and hydralazine), particularly when IV access is not in place. In most cases, use of immediate-release oral nifedipine will be safe and well tolerated; however, there is a risk of an acute, precipitous fall in blood pressure, which may result in a reduction in uteroplacental perfusion. The immediate-release preparations are also associated with a higher incidence of headache and tachycardia. In nonpregnant adults, the package insert states that "nifedipine capsules should not be used for the acute reduction of blood pressure.






















![PIHTN.pptx is increase of blood pressure during pregnancy of the mother [{}]#...](https://cdn.slidesharecdn.com/ss_thumbnails/pihtn-240806061903-454708ae-thumbnail.jpg?width=640&height=640&fit=bounds)












































