Pharmacotherapy of Chronic Renal Failure.pptx
•Download as PPTX, PDF•
0 likes•10 views

Pharmacotherapy of Chronic Renal Failure

Recommended
More Related Content
Similar to Pharmacotherapy of Chronic Renal Failure.pptx
Similar to Pharmacotherapy of Chronic Renal Failure.pptx (20)
More from Sreenivasa Reddy Thalla
More from Sreenivasa Reddy Thalla (20)
Recently uploaded
Recently uploaded (20)
Pharmacotherapy of Chronic Renal Failure.pptx
- 1. Sreenu Thalla Associate Professor Department of Pharmacology
- 2. Introduction • Chronic kidney disease (CKD) is defined as the presence of kidney damage or an estimated glomerular filtration rate (eGFR) less than 60 ml/min/1.73m2, persisting for 3 months or more, irrespective of the cause. • It is a state of progressive loss of kidney function ultimately resulting in the need for renal replacement therapy (dialysis or transplantation). • Kidney damage refers to pathologic abnormalities either suggested by imaging studies or renal biopsy, abnormalities in urinary sediment, or increased urinary albumin excretion rates.
- 4. KDIGO (Kidney Disease Improving Global Outcomes)
- 5. • The improved classification of CKD has been beneficial in identifying prognostic indications related to decreased kidney function and increased albuminuria. • However, a downside of the use of classification systems is the possible over diagnosis of CKD, especially in the elderly.
- 7. Etiology • Diabetes mellitus type 2 (30% to 50%) • Diabetes mellitus type 1 (3.9%) • Hypertension (27.2%) • Primary glomerulonephritis (8.2%) • Chronic Tubulointerstitial nephritis (3.6%) • Hereditary or cystic diseases (3.1%) • Secondary glomerulonephritis or vasculitis (2.1%) • Plasma cell dyscrasias or neoplasm (2.1) • Sickle Cell Nephropathy (SCN) which accounts for less than 1% of ESRD patients in the United States
- 9. Epidemiology • The true incidence and prevalence of CKD are difficult to determine because of the asymptomatic nature of early to moderate CKD. • The prevalence of CKD is around 10% to 14% in the general population. • Similarly, albuminuria (microalbuminuria or A2) and GFR less than 60 ml/min/1.73 m2 have a prevalence of 7% and 3% to 5%, respectively. • Worldwide, CKD accounted for 2,968,600 (1%) of disability-adjusted life-years and 2,546,700 (1% to 3%) of life-years lost in 2012. • Kidney Disease Outcomes Quality Initiative (KDOQI) mandates that for labeling of chronicity and CKD, patients should be tested on three occasions over a 3-month period with 2 of the 3 results being consistently positive.
- 32. CKD may result from disease processes in any of the three categories: • Prerenal (decreased renal perfusion pressure) • Intrinsic renal (pathology of the vessels, glomeruli, or tubules- interstitium) • Postrenal (obstructive).
- 33. Mechanisms of Accelerated Progression of CKD • Systemic and intraglomerular hypertension • Glomerular hypertrophy • Intrarenal precipitation of calcium phosphate • Altered prostanoid metabolism • All these mechanisms lead to a histological entity called focal segmental glomerulosclerosis. • Clinical risk factors for accelerated progression of CKD are proteinuria, hypertension, black race, and hyperglycemia. • Also, environmental exposures such as lead, smoking, metabolic syndrome, possibly some analgesic agents, and obesity have also been linked to accelerated progression of CKD.
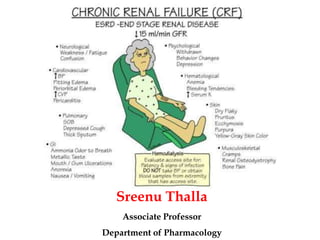
- 34. History and Physical • Nausea, Vomiting, Loss of appetite, Fatigue and weakness • Sleep disturbance, Oliguria, Decreased mental sharpness • Muscle twitches and cramps, Swelling of feet and ankles • Persistent pruritus, Chest pain due to uremic pericarditis • Shortness of breath due to pulmonary edema from fluid overload • Hypertension that's difficult to control Physical examination is often not helpful, but patients may have • Skin pigmentation • Scratch marks from pruritus • Pericardial friction rub due to uremic pericarditis • Uremic frost, where high levels of BUN result in urea in sweat • Hypertensive fundal changes suggesting chronicity
- 35. Differential Diagnosis • Acute kidney injury • Alport syndrome • Antigiomerular basement membrane disease • Chronic glomerulonephritis • Diabetic nephropathy • Multiple myeloma • Nephrolithiasis • Nephrosclerosis • Rapidly progressive glomerulonephritis • Renal artery stenosis