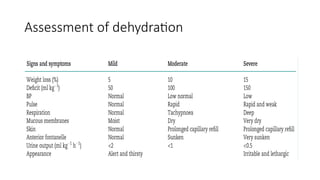
The document discusses pediatric perioperative fluid management, emphasizing the importance of intravenous fluid therapy before, during, and after surgery to maintain circulation and electrolyte balance. It outlines types of fluids, principles of fluid therapy, and the challenges of managing fluid therapy in newborns, noting that fluid overload can lead to significant complications. A retrospective cohort study is presented, highlighting the association between fluid overload in newborns after abdominal surgery and increased duration of ventilator support.

![Isotonic Solution
• They have tonicities close to that of plasma as termed ISOTONIC.
• Common examples are : 0.9% Saline, Ringer’s Lactate, D5-1/4NS and
Plasmalyte.
• Balanced electrolyte solutions- (low-[Cl–] crystalloids, which have
preserved ionic “balance” by replacing Cl– with lactate, gluconate, or
acetate) such as lactated Ringer’s solution or PlasmaLyte are most
commonly used for replacement.](https://image.slidesharecdn.com/pediatricsfluidmanagement-241118133421-f2e801d8/85/Pediatrics-Fluid-management-pptx-MUHIMBILI-9-320.jpg)

![Colloids
• Colloids contain homogeneous non-crystalline particles suspended in
balanced crystalloid or isotonic saline.
• These particles tend to remain within the bloodstream after infusion,
thus increasing intravascular oncotic pressure and expanding plasma
volume.
• Colloids are either artificial (hydroxyethyl starch [HES], gelatins and
dextrans) or derived from donated blood (albumin and fractionated
blood products).](https://image.slidesharecdn.com/pediatricsfluidmanagement-241118133421-f2e801d8/85/Pediatrics-Fluid-management-pptx-MUHIMBILI-14-320.jpg)

![CONT.
• Colloid solutions:
• During blood loss, some clinicians prefer to administer colloid (e.g. albumin) on a
1:1 volume basis until a transfusion threshold is met.
• We minimize colloid use due to insignificant hemodynamic benefits compared
with crystalloids.
• Blood transfusion:
• Red blood cells (RBCs) are used to replace blood loss when a transfusion
threshold is met.
• Decisions regarding transfusion of plasma derivatives (eg, fresh frozen plasma
[FFP]) are based on estimates of blood loss and evidence of abnormal
hemostasis.](https://image.slidesharecdn.com/pediatricsfluidmanagement-241118133421-f2e801d8/85/Pediatrics-Fluid-management-pptx-MUHIMBILI-19-320.jpg)

![Methodology cont..
• Statistical analysis
• Patient demographics and clinical characteristics were reported as median
(interquartile range [IQR]) and proportion (%) for continuous and categorical
variables, respectively.
• Odds ratio and 95% confidence interval were calculated using univariate logistic
regression analyses to quantify the association between adverse outcomes and
FO.
• Multivariable logistic regression was performed after adjusting for potential
confounders and other covariates based on the findings of the univariate analysis.
• R (v.4.0.3) using R-studio (v.1.3.1073) was used for statistical analysis, with p<.05
to be considered statistically significant.](https://image.slidesharecdn.com/pediatricsfluidmanagement-241118133421-f2e801d8/85/Pediatrics-Fluid-management-pptx-MUHIMBILI-42-320.jpg)
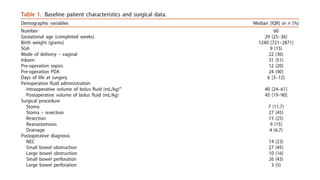
![Results
• Between January 2017 and June 2019, 83 newborns underwent abdominal
surgery.
• Sixty patients were included in this study, with a median [IQR] gestational age
of 29 weeks [25–36] and a median [IQR] birth weight of 1240 g [721–2871].
• Surgery was conducted at a median [IQR] of 6 DoL [3–12], with 32 patients
having surgery before 7 DoL and 28 patients having surgery on or after 7 DoL
• The actual median daily fluid intake was 178 mL/kg on postoperative days 0–2
and 163 mL/kg from postoperative days 3 to 7, which were significantly higher
than the median prescribed fluid volume of 145 mL/kg (p<.01).
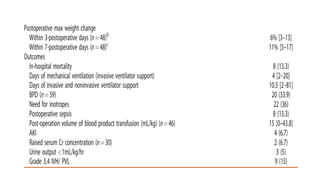
• The maximum median [IQR] percentage of weight change was 6% [3–13] and
11% [5–17] in postoperative days 3 and 7, respectively](https://image.slidesharecdn.com/pediatricsfluidmanagement-241118133421-f2e801d8/85/Pediatrics-Fluid-management-pptx-MUHIMBILI-43-320.jpg)