Pediatric Ophthalmology Concerns after Retinopathy of Prematurity. A lecture given at the Joint Asia Pacific Vitreo-Retina Society-Philippine Academy of Ophthalmology Congress, SMX Convention Center, December 11, 2025
Zapanta VQ, Monzon-PajarilloAK and Santiago APD for the Philippine Pediatric Society (PPS), Philippine
Society of Newborn Medicine (PSNbM) and the Philippine Academy of Ophthalmology– Retinopathy of
Prematurity Working Group (PAO-ROPWG). Retinopathy of Prematurity Philippine Preventive Care Plan Strategy.
A Consensus Statement of the Philippine Pediatric Society (PPS), Philippine Society of Newborn Medicine
(PSNbM) and the Philippine Academy of Ophthalmology – Retinopathy of Prematurity Working Group (PAO-
ROPWG). Phil J Ophthalmol 2020; 45(2): 58-64.
6.
Zapanta VQ, etal for the PSNbM, PAO-ROPWG (2020). Retinopathy of Prematurity Philippine Preventive Care Plan Strategy. A
Consensus Statement of the Philippine Pediatric Society (PPS), Philippine Society of Newborn Medicine (PSNbM) and the Philippine
Academy of Ophthalmology – Retinopathy of Prematurity Working Group (PAO-ROPWG). Phil J Ophthalmol 2020; 45(2): 58-64.
CONTROL
BIGGER PRETERMS, NoROP
(Underrepresented)
Very small
preterms, no ROP
Preterm w ROP
No treatment
Preterm w ROP
With treatment
17.
● Odds ofamblyopia increased with
younger GA
</= 28 wks compared to term
● Placental insufficiency tripled
amblyopia odds
● ROP with treatment: 15x odds
18.
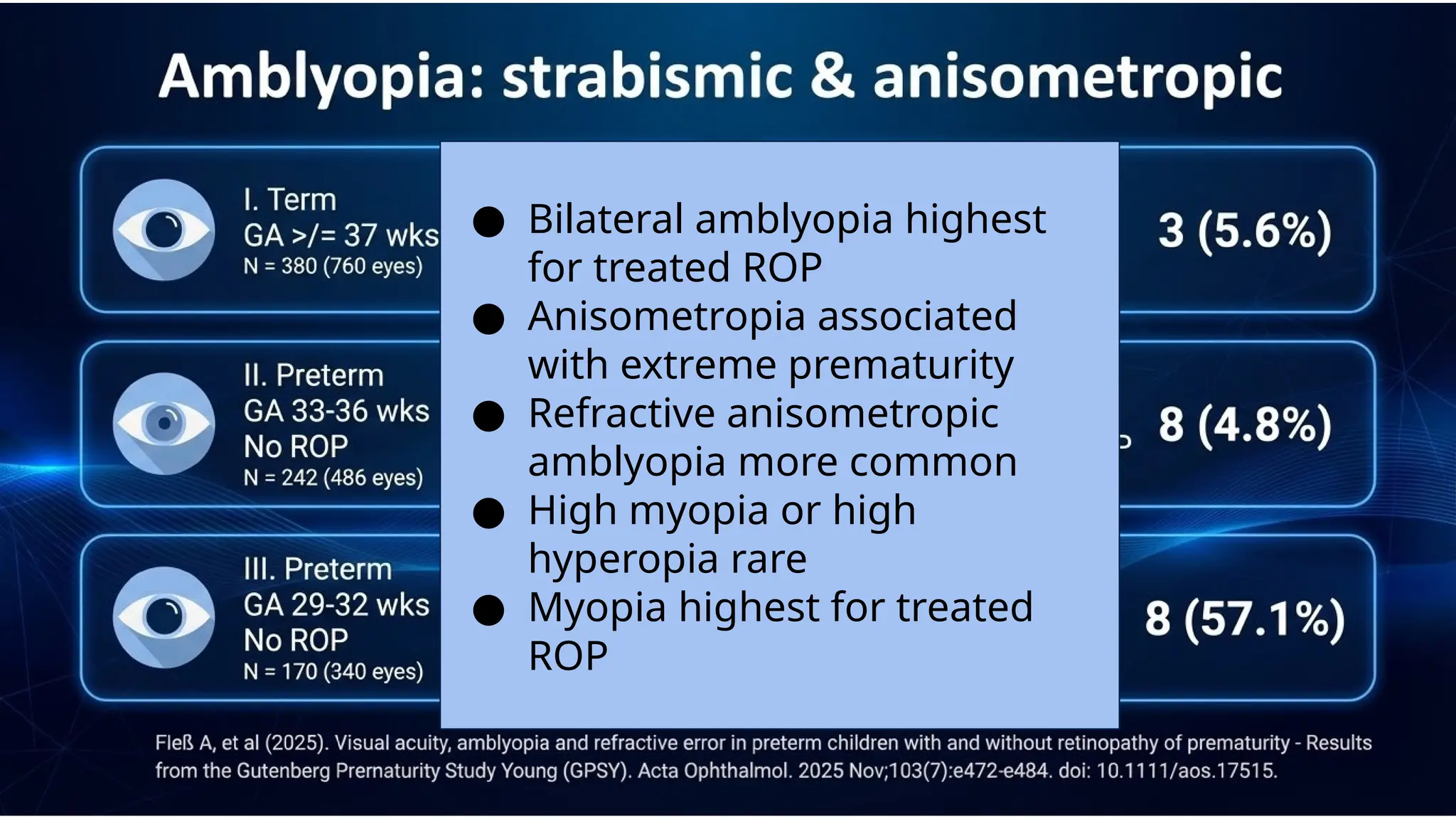
● Bilateral amblyopiahighest
for treated ROP
● Anisometropia associated
with extreme prematurity
● Refractive anisometropic
amblyopia more common
● High myopia or high
hyperopia rare
● Myopia highest for treated
ROP
Strab: 3 (2.1%)
Nys:1 (1.5%)
Strab: 9 (6.6%)
Nys: 2 (1.5%)
Strab: 16 (17.4%)
Nys: 4 (4.3%)
Strab: 2 (11.1%)
Nys: 1 (5.6%)
Strab: 13 (27.1%)
Nys: 5 (10.4%)
Strab: 9 (60%)
Nys: 4 (26/7%)
STRABISMUS
● Esotropia (ET) more frequent than exotropia
● Most strabismus within first 10 years
NYSTAGMUS
● Perinatal adverse events strongest predictor (OR 15.8;
p=0.002)
38.
-42 eyes (25patients)
-mean logMar 0.83 (20/135) to 0.63 (20/85)
-myopic shift >/= 1D in 21 eyes (62%)
between age 5-8
-Stage 4A dominant eyes showed
improvement by age 5-8
-Stage 4B eyes: no significant BCVA
improvement
After Vitrectomy for Stage 4 ROP
1. Tachibana K, Iwahashi C, Kuniyoshi K, Kusaka S. Long-term visual function and refractive changes after vitrectomy for stage 4
retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2025 Jul;263(7):2041-2048. doi: 10.1007/s00417-025-06801-0. Epub 2025
Mar 22. PMID: 40119916; PMCID: PMC12373698.
https://drswatisinkar.com.au/
39.
● 61 eyes,42 patients
● retrospective
● 4 years follow up
● Mean decimal BCVA at follow up: 0.23 (20/100)
+- 0.25 (HM to 1.2)
● 23 (54%) BCVA 0.4 (20/50)
● Mean refractive error was −10.1 ± 5.0 D
● 37 eyes (75.5%) having high myopia (>−6.0 D).
Lens-sparing vitrectomy
(+ antiVEGF) for St 4A ROP
1. Iwahashi C, Kurihara T, Kuniyoshi K, Kusaka S. Long-Term Visual Prognosis of Patients Following Lens-Sparing Vitrectomy for Stage 4A
Retinopathy of Prematurity. Int J Mol Sci. 2023 Jan 26;24(3):2416
https://drswatisinkar.com.au/
40.
Cataracts in ROP
Systemi
c
Metabolicacidosis, sepsis
Post Treatment
03
01
Khokhar S, Surve A, Verma S, Azad S, Chandra P, Dhull C, Vohra R. Cataract in retinopathy of prematurity - A review. Indian J Ophthalmol.
2022 Feb;70(2):369-377
Complicated
cataract
02
Associated with RD/Stage 5
Cryo, Laser, AntiVEGF, Vitrectomy
TVL, Anterior Segment Ischemia, Uveal Effusion
Steroid Induced
41.
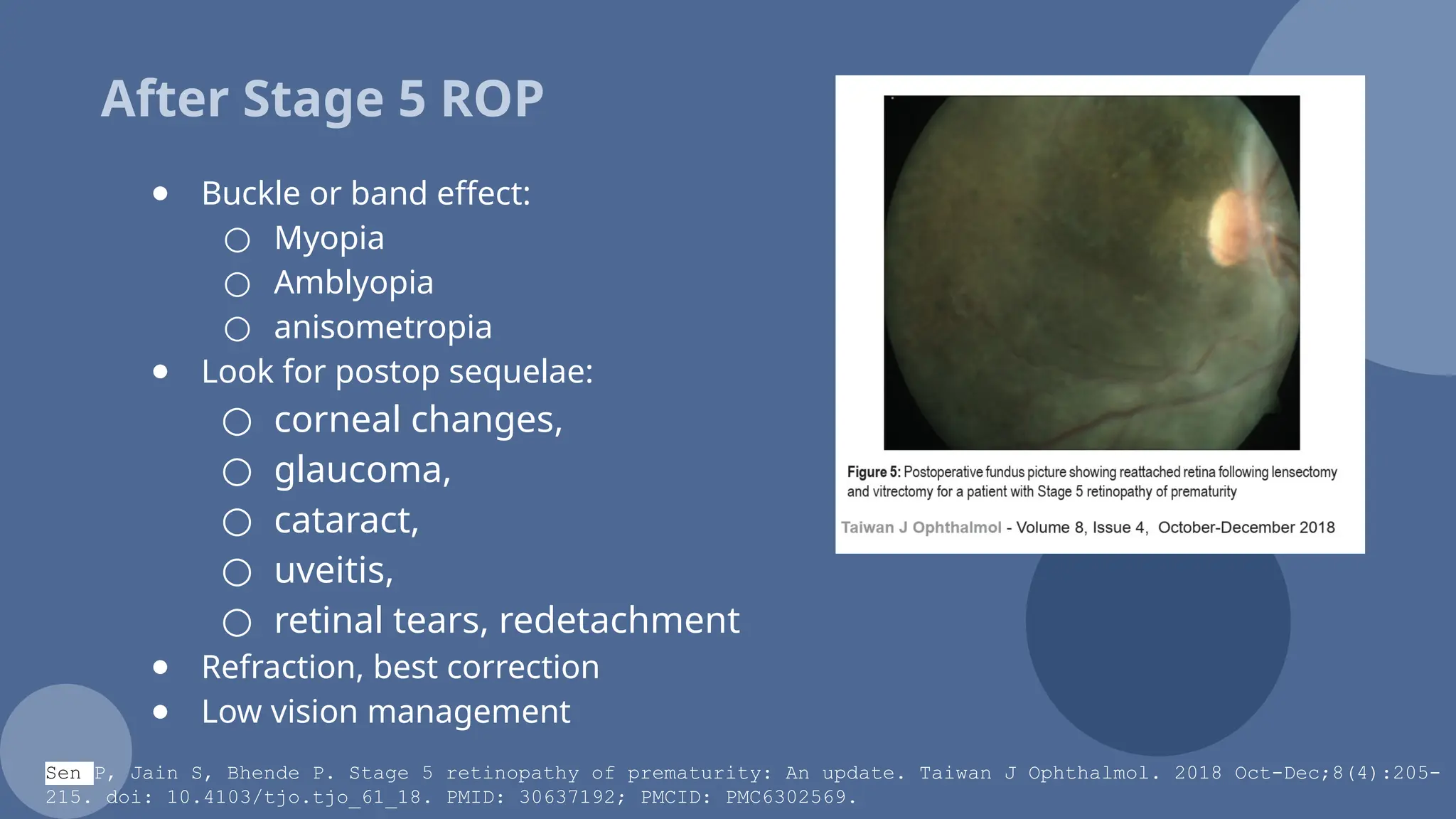
After Stage 5ROP
● Buckle or band effect:
○ Myopia
○ Amblyopia
○ anisometropia
● Look for postop sequelae:
○ corneal changes,
○ glaucoma,
○ cataract,
○ uveitis,
○ retinal tears, redetachment
● Refraction, best correction
● Low vision management
Sen P, Jain S, Bhende P. Stage 5 retinopathy of prematurity: An update. Taiwan J Ophthalmol. 2018 Oct-Dec;8(4):205-
215. doi: 10.4103/tjo.tjo_61_18. PMID: 30637192; PMCID: PMC6302569.
42.
Ophthalmic
Sequelae
Late
childhood,
Early
Adulthood
Myopia
(& other refractiveerrors)
Strabismus
Ocular hypertension,
glaucoma
Corneal aberrations
Retinal tears and detachments,
ERM, foveal anomalies
01
02
03
04
1. Downes RA, Rachitskaya AV. Ophthalmic sequelae of prematurity in late childhood and adulthood: A review. Clin Exp Ophthalmol. 2024
Apr;52(3):355-364.
CREDITS: This presentationtemplate was
created by Slidesgo, including icons by
Flaticon, infographics & images by Freepik
Thank
you
kidseyes@health-channel.com
Please keep this slide for attribution
https://www.voanews.com/
https://www.voanews.com/
Editor's Notes
#1 Good afternoon everyone. Thank you for the opportunity to talk to you about pediatric ophthalmology concerns after a Retinopathy of Prematurity or ROP diagnosis
#2 The only disclosure I have is that AI was used to beautify most slides in this deck
#4 The learner is expected to achieve the following outcomes at the end of this session
#5 The ROP Preventive care plan strategy is published in the PJO, as well as the VRSP
#6 Key recommendations for screening include screening babies born less than or equal 32 wks, or with a birth weight less than or equal to 1500g, or preterms less than 36 weeks with STOP… sepsis, transfusion, oxygen use, and prematurity course that is less than comforting
#7 The gist of this lecture are the following pedia ophtha concerns: EOR< Strabismus, amblyopia, Laser and anti VEGF sequelae, retinal surrey sequalae, and lean opacity that can be a sequelae of both the disease or treatment
#8 ohannes Gutenberrg University, in recent years have conducted the Gutenberg Prematurity Eye Study, and more recently the Gutenberg Prematurity Study Young.
#9 In both studies they evaluated visual acuity, refraction, presence of amblyopia, lens opacification, strabismus, nystagmus, and their vision related quality of life
#10 The Gutenberg Prematurity study young is an ongoing retrospective cohort, where 1898 eyes are included.
Children born preterm between 2003 to 2018, were evaluated at age 4-17
#12 They have 6 categories
Term,
3 groups of Preterms without ROP 33-36 wks, Preterm 29-32 wks, and less than 28 wks
2 groups of preterms with ROP: treated and non treated
#17 Odds of amblyopia increased with younger GA
</= 28 wks compared to term
Placental insufficiency tripled amblyopia odds
ROP with treatment: 15x odds
#18 Bilateral amblyopia highest for treated ROP
Anisometropia associated with extreme prematurity
Refractive anisometropic amblyopia more common
High myopia or high hyperopia rare
Myopia highest for treated ROP
#19 For strabismus, notice that groups 4, 5, 6… small preterms, and thos e with ROP showed a higher incidence. Highest for preterms treated ROP
#21 Top left shows graphical the strabismus in patients with treated ROP
Top right showed the type of strabismus, with esotropia more common
Bottom left or C, shows strabismus as it relates to ROP stage, most common in St 3
Bottom right shows visual acuity in log mar (0 is 20/20), vision being weakest for treated ROP
#22 Nystagmus is also most common in the treated ROP group
#24 You see this again in this logmar representation…
Treated ROP eyes, for stage 3-5 showing higher prevalence
#25 In the Gutenberg prematurity study, this was very similar to the first prematurity study young, except they studied adults age 18-52…
Their studies stress the important of lifelong monitoring of preterm babies
#26 The same grouping
1 is control
3 grps of preterms without ROp
And 2 grps with ROP, one treated and one non treated
#27 This were the prevalence of strabismus and nystagmus, more prominent in the group with ROP, esp in the group that was treated
#28 Esotropia (ET) was more frequent than exotropia
Most strabismus occur within first 10 years
Perinatal adverse events strongest predictor (OR 15.8; p=0.002) of nystagmus with odds ration of 16
#29 Multivariate regression analysis showed an OR of close to 1 for low GA; and varying refractions, with OR of 3-10 for the different refractive errors. Note that there is myopia that correlated with strabismus
#30 In general, ROP w treatment had poorest visual outcome and socioemotional QoL
AMlbyopia more frequent in preterms
Distance vision correlated with gestational age, birth weight, ROP treatment, ROP, and perinatal adverse events
VR QOL lower in preterms
#31 The gutenberg studies have also been reporting about the cornea, biometry, fovea, optic nerve of these preterms who are now all grown.
#32 These are the papers of the Gutenberg studies I used for this report
#34 Many studies support that antiVEGF has a lower risk of myopia and better refractive outcomes
#35 But there are studies that report no difference between the 2
#36 Further, there s a study that showed treated and non treated eyes did not show any difference in outcomes
#37 There are the references for Antivegf vs laser portion
#38 What happens after stage 4 ROP… myopic shift of more than 1D is documented in 60%
Continued improvement in vision over time observed for stage 4A but not for stage 4B
#39 BcVA is about 20/100; with a mean refractive error of -10D. More than 75% have high myopia
#40 Cataracts in ROP can be from systemic associations, such as metabolic acidosis and sepsis; complicated cataracts from RD or Stage 5 ROP, and post treatment
#41 After stage 5 ROP, the band can cause myopia, amblyopia, anisometropia
As PO, we also look for other problems so that they can be addressed or referred as necessary
Refraction need to be performed
And Low vision referral is often required
#42 Ophthalmic sequelae is outline in this slide.. And can come or be recognized years later.
#43 If This lecture can achieve one thing, it should be the realization that a diagnosis of ROP, regardless of wether the patient is treated or note, requires a lifelong ophthalmic care and follow-up