Downloaded 11 times
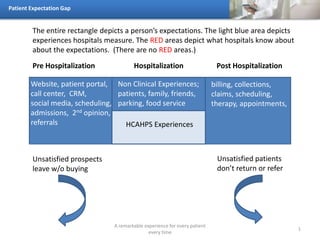

The document discusses the patient expectation gap in healthcare, emphasizing the importance of delivering a remarkable experience for every patient at all stages of hospitalization. It highlights various aspects of patient experiences, including non-clinical factors like food service and call centers, as well as the consequences of unmet expectations, such as patients not returning or referring others. The document visually represents the gap between what is measured by hospitals and what is actually known about patient expectations.

































