Download to read offline
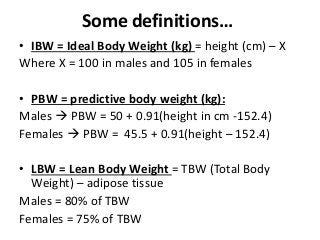
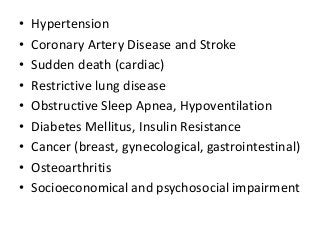
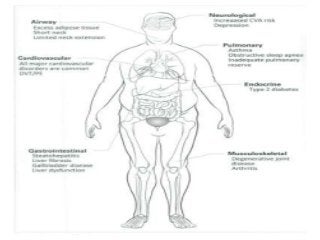
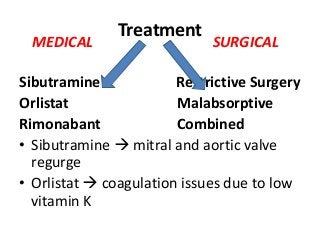
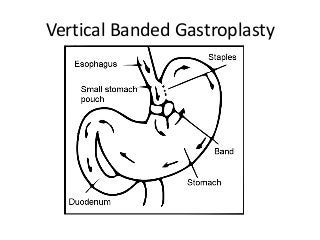
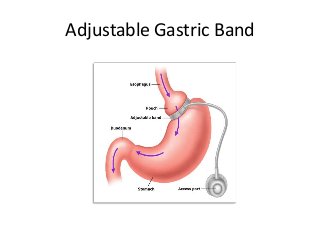

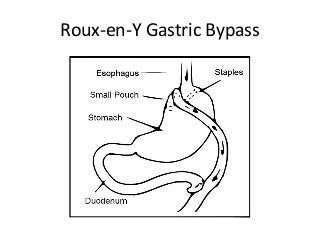
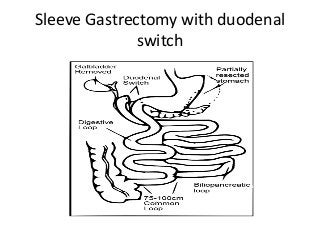



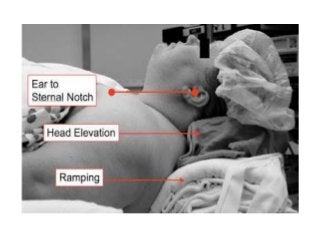
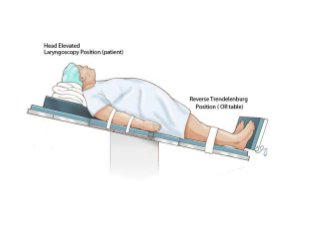




This document discusses bariatric surgery and considerations for anesthesiologists. It begins by defining obesity and its health risks. It then discusses the types of bariatric surgeries available and their indications and contraindications. Key considerations for anesthesiologists are the pathophysiological changes in obese patients that affect respiratory, cardiovascular, gastrointestinal and other body systems. Proper positioning, airway management, and drug dosing tailored to the patient's lean body weight versus total body weight are emphasized. Close monitoring is needed during induction, maintenance and emergence from anesthesia due to risks like regurgitation and hypoxemia.















































