Download as PDF, PPTX












![STAT | continued
THE NAVY’S FIRST AVIATION PA MAKES HISTORY
Lt. William Grisham, U.S. Navy, became the Navy’s first Aviation PA in a historic
“winging”ceremony on Sept. 21, 2016, in Pensacola, Fla. He now serves as a
Navy Aerospace Medical Institute (NAMI) staff member and treats naval aviators
and aviation flight crew patients.
His journey started five years ago, when he received the opportunity to stay
in Atsugi, Japan, and work in aerospace medicine with Carrier Air Wing Five. His
incredible work with flight surgeons set the stage for a new PA training program
with NAMI. The six-month program consists of pre-flight indoctrination, abbre-
viated flight training combined with aerospace medicine topics in primary care,
acute care, occupational health, preventive medicine and naval aviation safety.
“Lt. Grisham’s designation as the first Aeromedical PA is great for the fleet,
Navy Medicine and the Medical Service Corps’Physician Assistant community,”
said Capt. John Wyland, U.S. Navy, who was the officer in charge of NAMI at the
time of Grisham’s appointment to the program.“Aerospace Medicine [PAs] will
serve as invaluable flight surgeon extenders in areas of direct patient care, pre-
ventive medicine, safety and readiness. They will fill critical operational billets,
and the experience they receive should enhance their ability to serve in future
leadership positions.”
CMS OFFERS OPTIONS FOR PACE OF
PARTICIPATION IN QPP PROGRAM
On September 8, CMS released a blog post describ-
ing their plans to permit flexibility in the pace of
implementation of the Quality Payment Program
(QPP) for 2017. The QPP implements the Merit-
Based Incentive Payment System and the Advanced
Alternative Payment Model provisions contained
in the Medicare Access and CHIP Reauthorization
Act, commonly known as MACRA. While techni-
cally not a delay in the QPP, this flexibility will offer
health professionals more time to meet QPP pro-
gram requirements.
In the blog post, CMS offered four potential
tracks for the QPP’s first year:
Option 1 – allows health professionals to test the
QPP by submitting limited data, and thereby
avoiding a negative payment adjustment, and
ensure the system is working prior to broader
participation in 2018 and 2019.
Option 2 – allows for participation for part of the
calendar year and the potential to qualify to
receive a small positive payment adjustment.
Option 3 – allows professionals to submit QPP
information for the full 2017 calendar year
to qualify for a modest positive payment
adjustment.
Option 4 – allows for participation in an Advanced
Alternative Payment Model in 2017 for a 5 per-
cent incentive payment in 2019.
CMS plans to release its final rule on the entire
QPP before November 1. Until then, please visit
AAPA’s QPP webpage to learn more. For more infor-
mation on the QPP and MACRA, see the September
issue of PA Professional.
NEW AAPA REPORT: PA SALARIES
ON THE RISE
The median base salary for PAs is continuing to rise
faster than the rate of inflation, according to the
new 2016 AAPA Salary Report. Despite only a slight
increase in the cost of living in the past year, the
median base salary for PAs increased 3.4 percent
and the median hourly wage increased 7.8 percent.
Available free to AAPA fellows, student members
and retired members, the salary report includes the
most detailed PA compensation and benefits infor-
mation available. It
features data on base
salary, bonuses and
hourly wages—broken
out by region, state,
experience, specialty,
employer type, work
setting and years of
experience. Download
the report here.
2016 AAPA
Salary Report
COURTESYOFU.S.DEFENSEDEPARTMENT
PA PROFESSIONAL | OC TOBER 2016 | AAPA.ORG | 17](https://image.slidesharecdn.com/b73bec67-272c-405a-9f4d-6d63847ec437-161017161254/85/PA_Pro_October_2016_HR_final-19-320.jpg)









![FEATURE STORY, continued
Ortho”clinic in 2005. Many of the more than 100 clinics using the Prompt
Ortho model operate under a licensing agreement with Mohnickey’s com-
pany, Prompt Orthopedic Clinics, LLC. More than 80 of these clinics are
directly affiliated with the company, and these carry one of the Prompt
brands, but Mohnickey has also consulted on more than 40 additional
clinics, which adapted the model to their particular needs and may be
part of other healthcare systems.
“We help each practice set up the model that is right for them,”
Mohnickey says. But what all the clinics have in common is that PAs are
central to the practice.“Our model makes the PA the primary provider in
the practice,”Mohnickey says.“The PA is the gatekeeper; they will see and
treat all the nonsurgical patients.”PAs with experience in orthopaedics are
ideally suited to this role, according to
Mohnickey.“A well-seasoned PA under-
stands the surgical side and the primary
care aspect of [musculoskeletal care],”
he says.
About one in six visits to an urgent care
center involve a musculoskeletal injury,
according to Mohnickey, and about 70
percent of these will be referred to an
orthopaedist. In the orthopaedic urgent
care clinics, fewer than 20 percent of
patients are referred for potential surgery,
25 percent are referred to physical or occupational therapy and
another 18 percent are referred for additional imaging.
There is a clear need for the clinics, agrees Mike Harvey, a PA
who manages five OrthoIndy orthopedic urgent care clinics in the
Indianapolis area.“In our area, nobody manages musculoskeletal
problems as well as an orthopedic practice,”he says.“But the ortho
surgeons should be spending their time seeing surgical cases. And the
days when primary care doctors managed orthopedic care are dwindling.
So we wanted to create an option for patients to get high quality musculo-
skeletal care.”
The ortho clinics are set up for specialized orthopedic care in a way that
general urgent care centers are not, Harvey notes.“The main thing we offer
is the musculoskeletal expertise. If you go to a regular urgent care they will
do an X-ray and splint you … sometimes they don’t do the best job with
immobilization or have the right crutches or braces on hand. We can do all
that, and if they do need to see a surgeon we can expedite getting them
and appointment.”
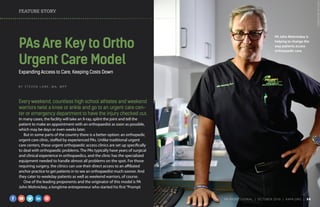
Mohnickey talking with PA
Heather Gehnke about the
new clinic. He wants PAs to
change the way they think
about practice setting.
PA Mike Harvey
PHOTOBYBENTORRES
COURTESYOFMIKEHARVEY
PA PROFESSIONAL | OC TOBER 2016 | AAPA.ORG | 35](https://image.slidesharecdn.com/b73bec67-272c-405a-9f4d-6d63847ec437-161017161254/85/PA_Pro_October_2016_HR_final-37-320.jpg)




This article discusses AAPA's political action committee (PA PAC) and addresses five common misconceptions. It explains that PA PAC is important for supporting federal candidates who understand issues vital to PAs. However, some PAs incorrectly believe that AAPA has plenty of funds or that individual contributions are not needed. The article clarifies that individual contributions are essential because AAPA cannot use membership dues or solicit non-members. It emphasizes that every contribution helps elevate the PA profession's voice in Congress, regardless of amount.












































