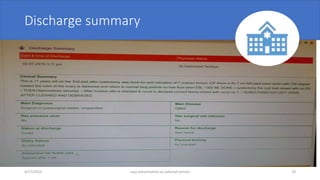
In this case, the patient presented with acute abdominal pain and was found to have a large ovarian cyst with absent Doppler flow on ultrasound concerning for ovarian torsion. She underwent an emergency laparotomy which confirmed torsion of the left ovary and cyst. The ovary appeared non-viable so a cystectomy was performed. Her postoperative course was uncomplicated. Overall this case highlights the importance of timely surgical intervention for suspected ovarian torsion to assess ovarian viability and prevent potential loss of the ovary.