Download to read offline

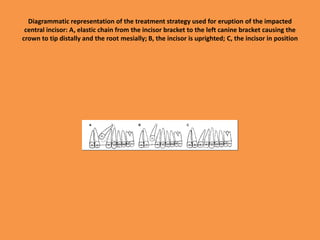


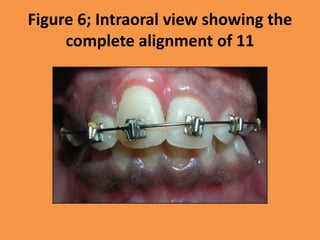
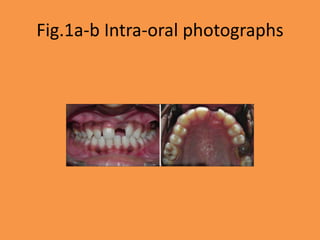
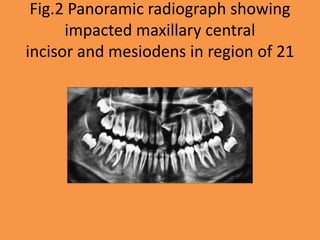
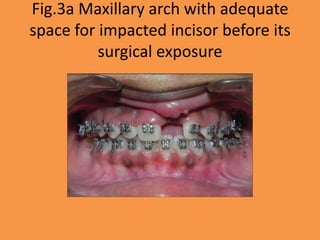
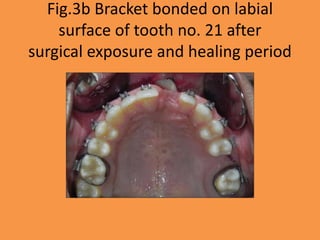
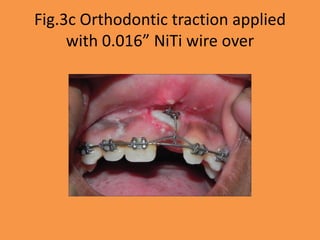
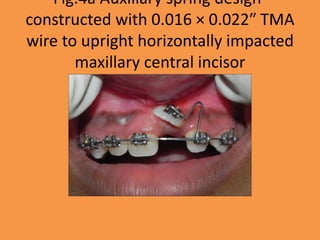
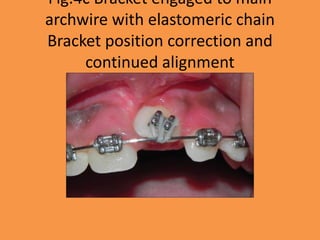







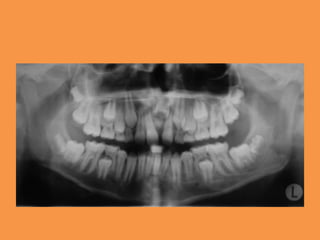
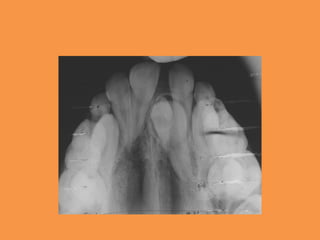
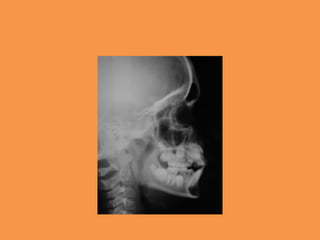








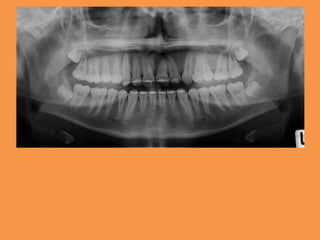
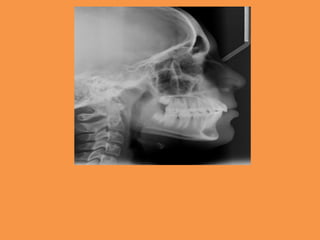

The document discusses the orthodontic management of impacted central incisors in a 10-year-old female patient, detailing various treatment options and techniques, including space creation, surgical exposure, and orthodontic traction. It highlights the importance of understanding the causes of impaction, such as supernumerary teeth, and outlines potential treatments ranging from extraction to autotransplantation. The author emphasizes the necessity of ongoing periodontal care following successful treatment to prevent relapse.

















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



