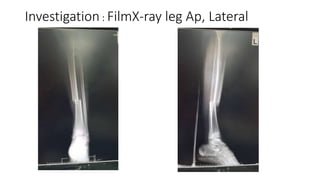
The document details the case of a 12-year-old boy who suffered an open fracture of the left tibia following a motorcycle accident. It outlines the clinical assessment, including vital signs and physical examination, as well as the Gustilo and Anderson classification for the type of fracture. Management recommendations are provided, including antibiotic therapy and surgical intervention strategies.