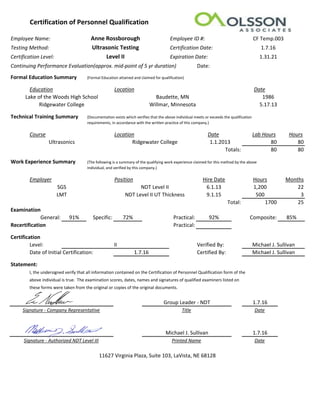
- Anne Rossborough holds NDT Level II certification in ultrasonic testing, which expires on January 31, 2021. She received this certification from Olsson Associates on January 7, 2016.
- She has an associate's degree from Ridgewater College in ultrasonic testing and work experience of over 25 months in the field working for two employers.
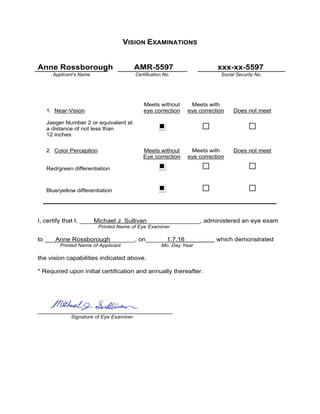
- Her most recent eye exam on January 7, 2016 demonstrated that she meets the vision requirements for NDT work both with and without eye correction.