Download to read offline
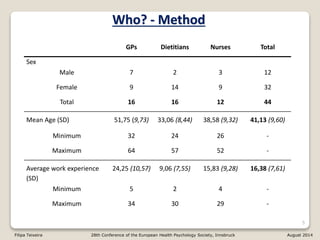
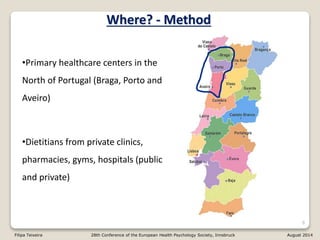

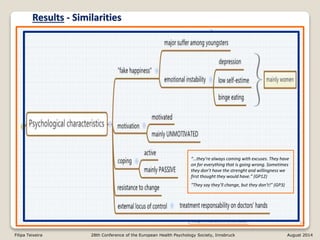
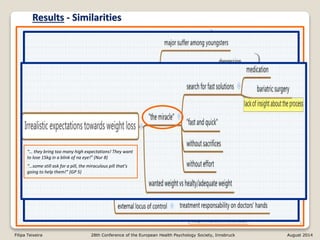
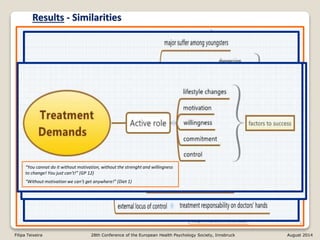
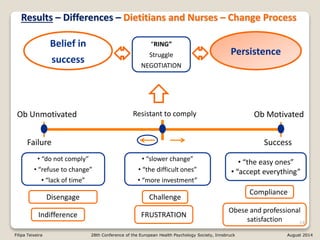
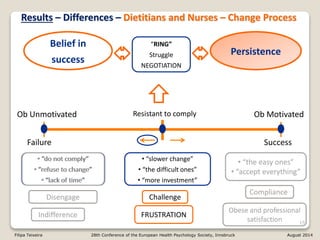
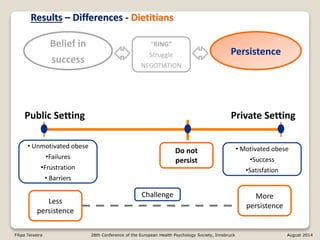
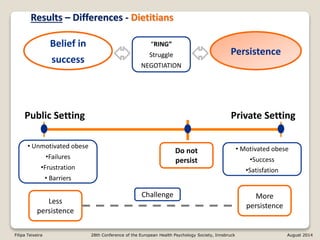
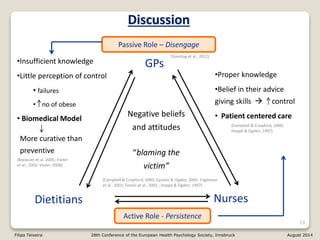



1) The document summarizes a study comparing the views of general practitioners, dietitians, and nurses on obesity in Portugal. 2) The professionals generally saw obese patients as unmotivated and making excuses, but dietitians and nurses were more persistent in treatment compared to general practitioners who tended to disengage. 3) The study highlights differences in views that could impact treatment effectiveness, such as general practitioners viewing obesity management passively while dietitians believed in their ability to facilitate change.















































