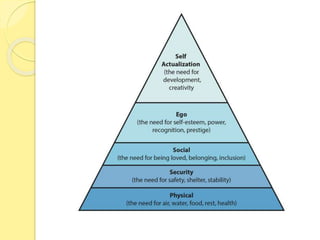
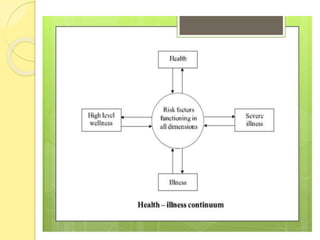
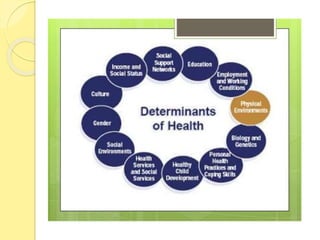
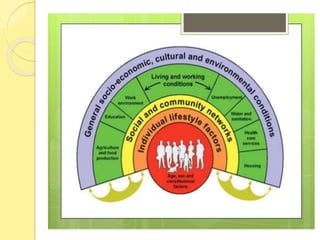
The document discusses concepts of health, wellness, illness, and factors that influence health. It defines health as a state of complete physical, mental, and social well-being, not just the absence of disease. Wellness refers to overall well-being and is plotted on a continuum from illness to optimal wellness. Illness is defined as a disease or period of sickness. Factors influencing health include biological, environmental, lifestyle, and psychological factors. The determinants of health encompass the social environment, physical environment, and individual behaviors and characteristics. Illness can impact patients and families by causing changes to roles and increasing stress and economic strain.













































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















