
More Related Content
Similar to Nhsla 2
Similar to Nhsla 2 (11)
Nhsla 2
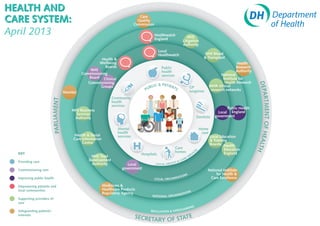
- 1. Care Quality Commission Healthwatch England NHS Litigation Authority Local Healthwatch NHS Blood Health & & Transplant Wellbeing Health Boards Public Research NHS health Authority Commissioning services National Board Clinical Institute for Commissioning Health Research DEPA & PATIEN Groups BLIC TS GP NIHR clinical PU surgeries research networks Monitor RT Community PARLIAMENT health MENT OF HEA services Public Health NHS Business Services Local England Authority Dentists government Mental Home health care Health & Social services Local Education Care Information & Training Centre LTH Boards Health Care S Education KEY homes I CE England Hospitals RV NHS Trust SE Development RE Providing care CA H& Authority Local LOCAL HEALT government Commissioning care National Institute S for Health & TION Care Excellence Improving public health LOCAL ORGANISA Empowering patients and Medicines & local communities Healthcare Products N S Regulatory Agency ATIO NATIONAL ORGANIS Supporting providers of care ING ARD Safeguarding patients’ REGULATION & SAFEGU interests SECRET E ARY OF STAT