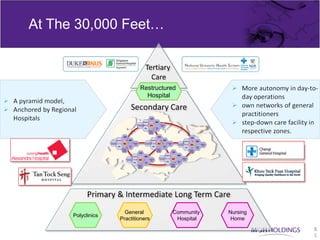
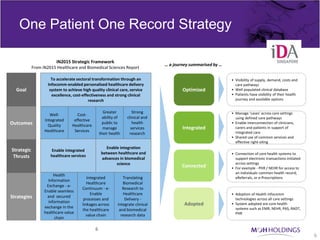
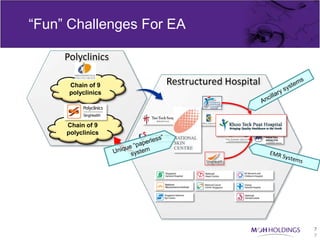
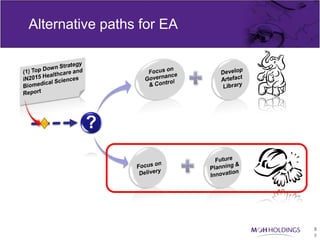
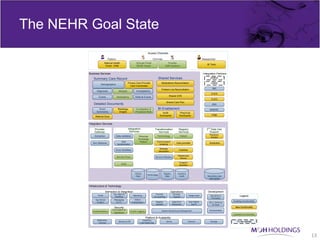
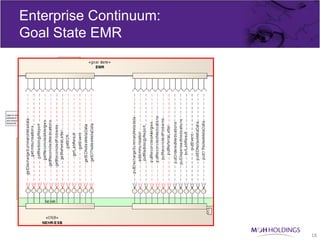
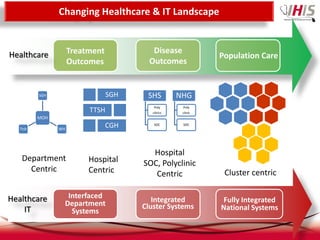
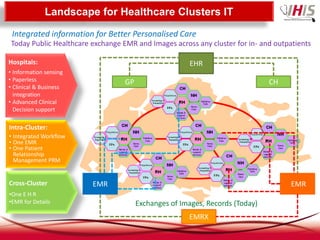
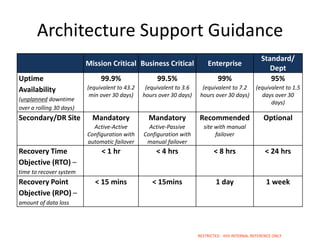
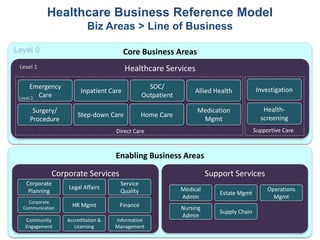
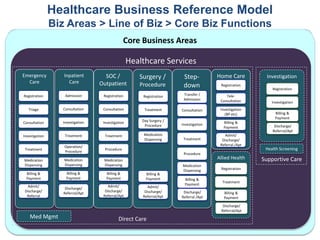
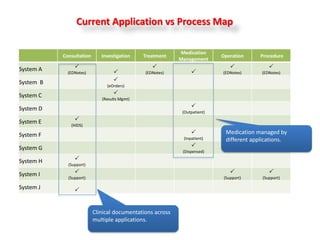
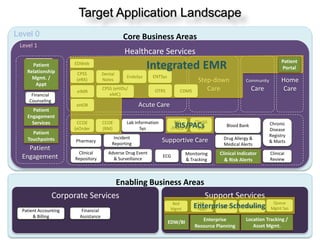
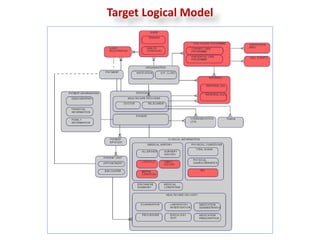




The document discusses two different architectures - the current architecture and a goal state architecture. The current architecture lacks integration between different care settings. The goal state architecture aims to improve integration through a shared patient record, standardized clinical data exchange, and defined care pathways that can manage patient cases across different care settings. It outlines strategies like enabling integrated healthcare services, adopting health infocomm technologies, and connecting core health systems to support the goal state architecture.




































![Globalization And A Changing World[1]](https://cdn.slidesharecdn.com/ss_thumbnails/globalization-and-a-changing-world1-1203529702448423-3-thumbnail.jpg?width=640&height=640&fit=bounds)















































