Download to read offline
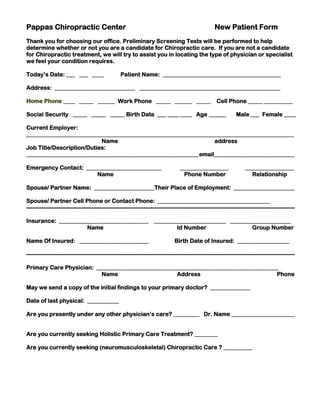
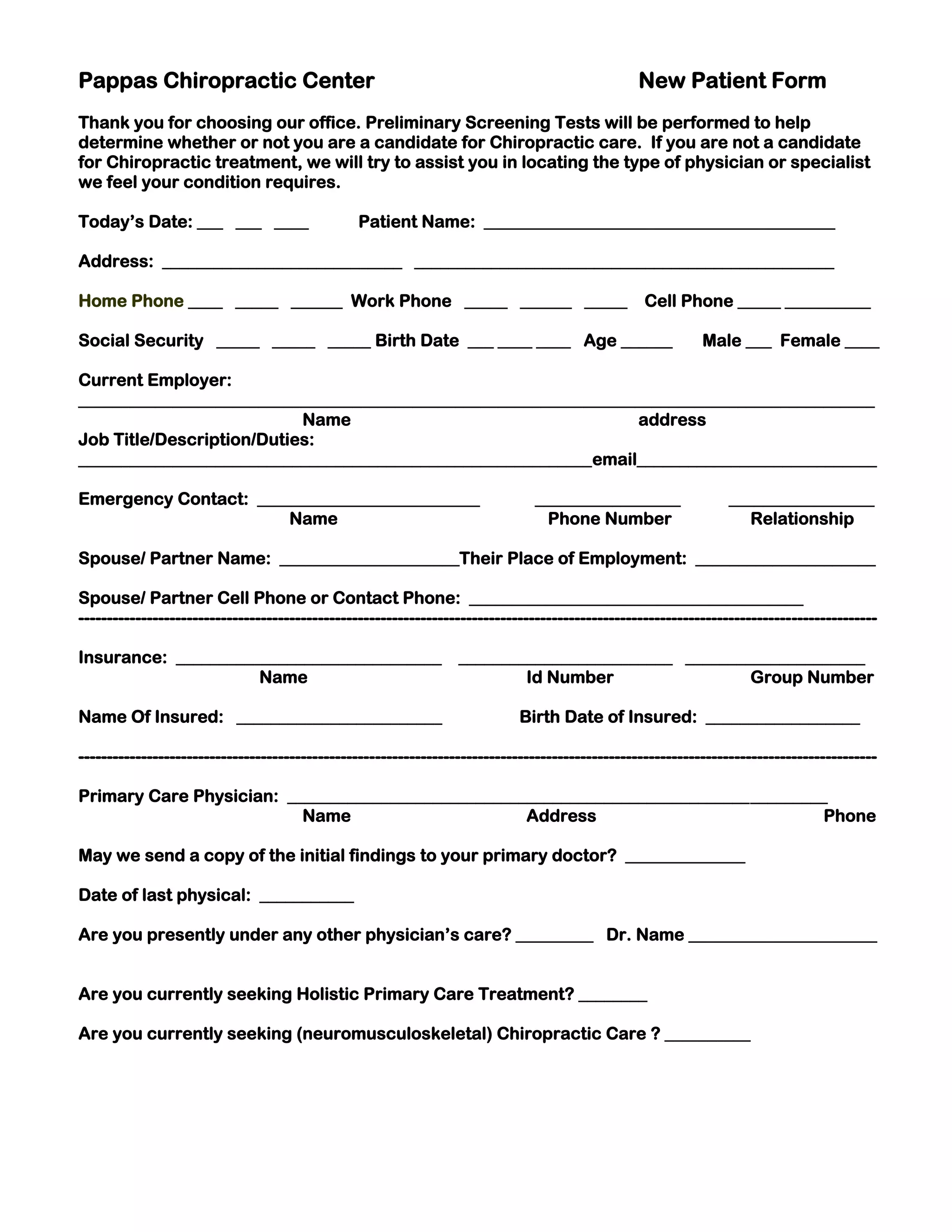
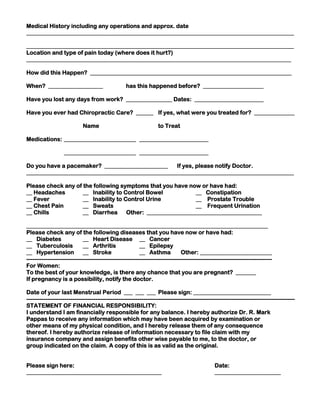

This new patient form collects information such as contact details, insurance, medical history, and current symptoms from a new patient of Pappas Chiropractic Center. Preliminary screening tests will be done to determine if chiropractic care is suitable, and if not, the patient will be referred to another physician. The form requests details on insurance, primary care physician, current and past medical conditions, current pain levels and locations, and authorizes the chiropractic center to file insurance claims and receive medical records from other providers.






























