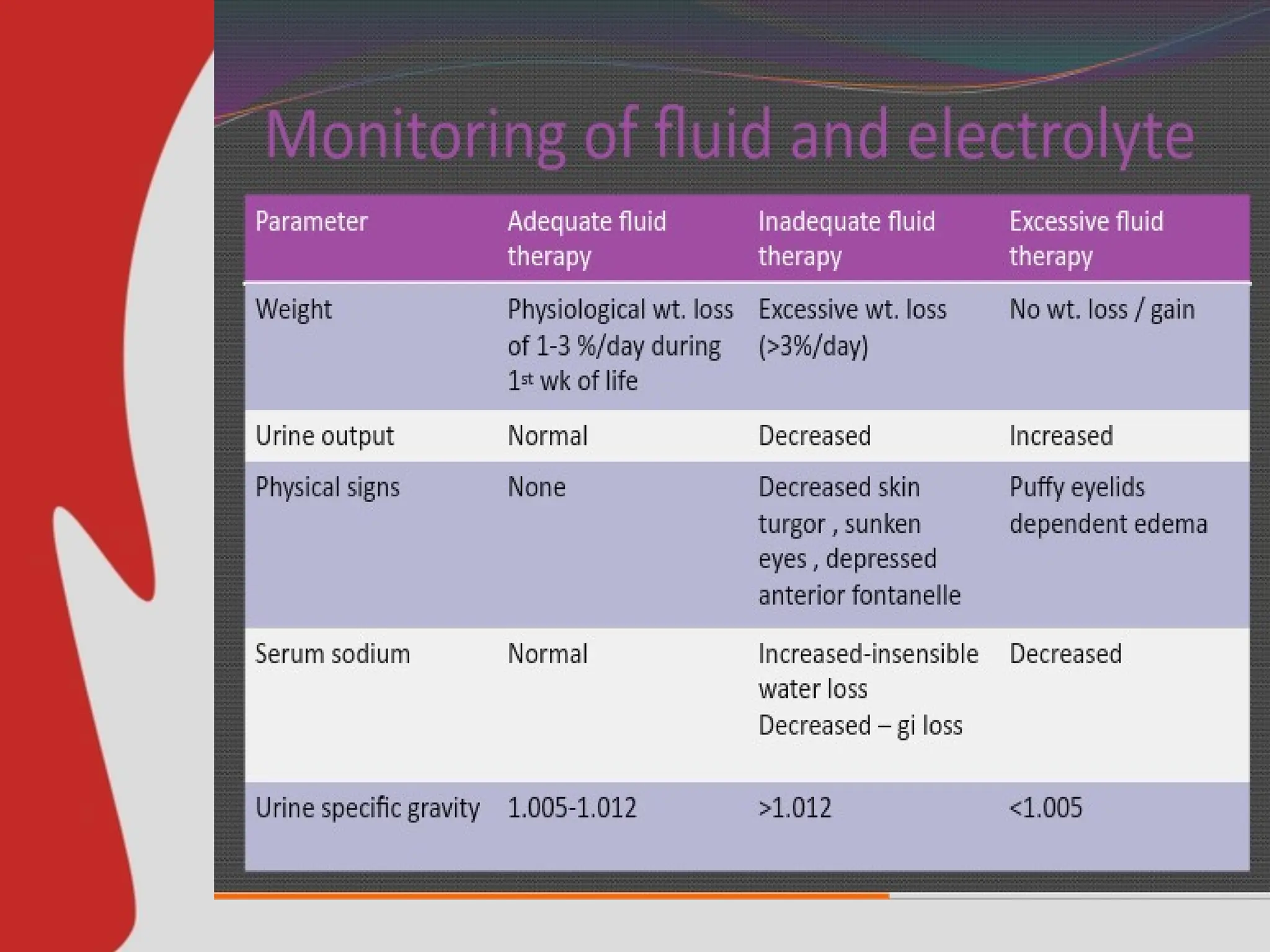
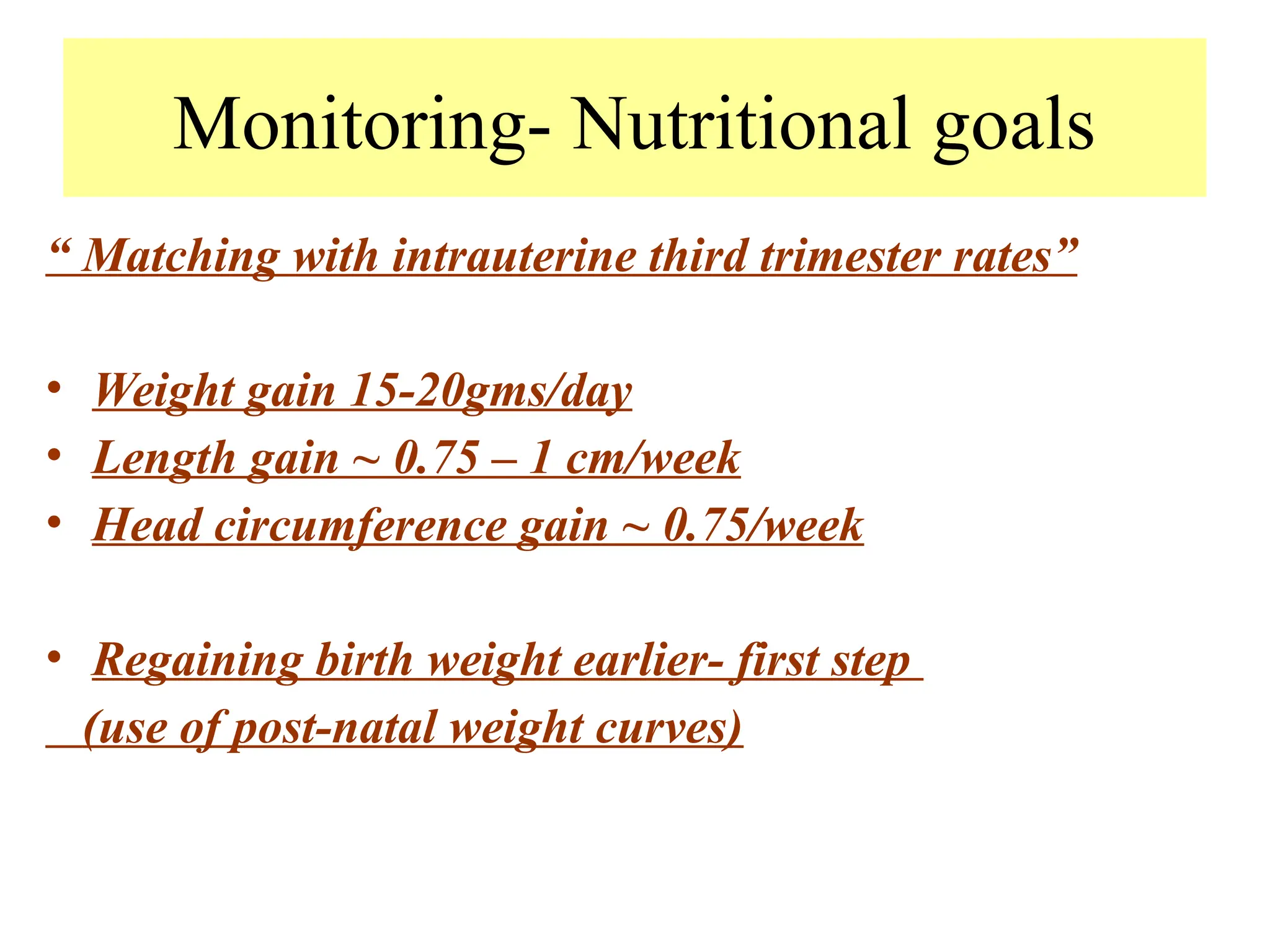
Proper nutrition is crucial for neonatal well-being, particularly for preterm and low birth weight infants due to their unique challenges such as immature gastrointestinal function and higher risk of complications. Strategies include early parenteral nutrition, gradual transition to enteral feeding, and continuous monitoring of growth parameters to optimize development. Addressing these nutritional needs is essential for improving growth velocity and long-term cognitive outcomes.